
Autoeczematization (Id Reaction) — MCQs

Pruritus is a feature of which of the following conditions?
Steroids are used in the Rx of the following diseases EXCEPT:
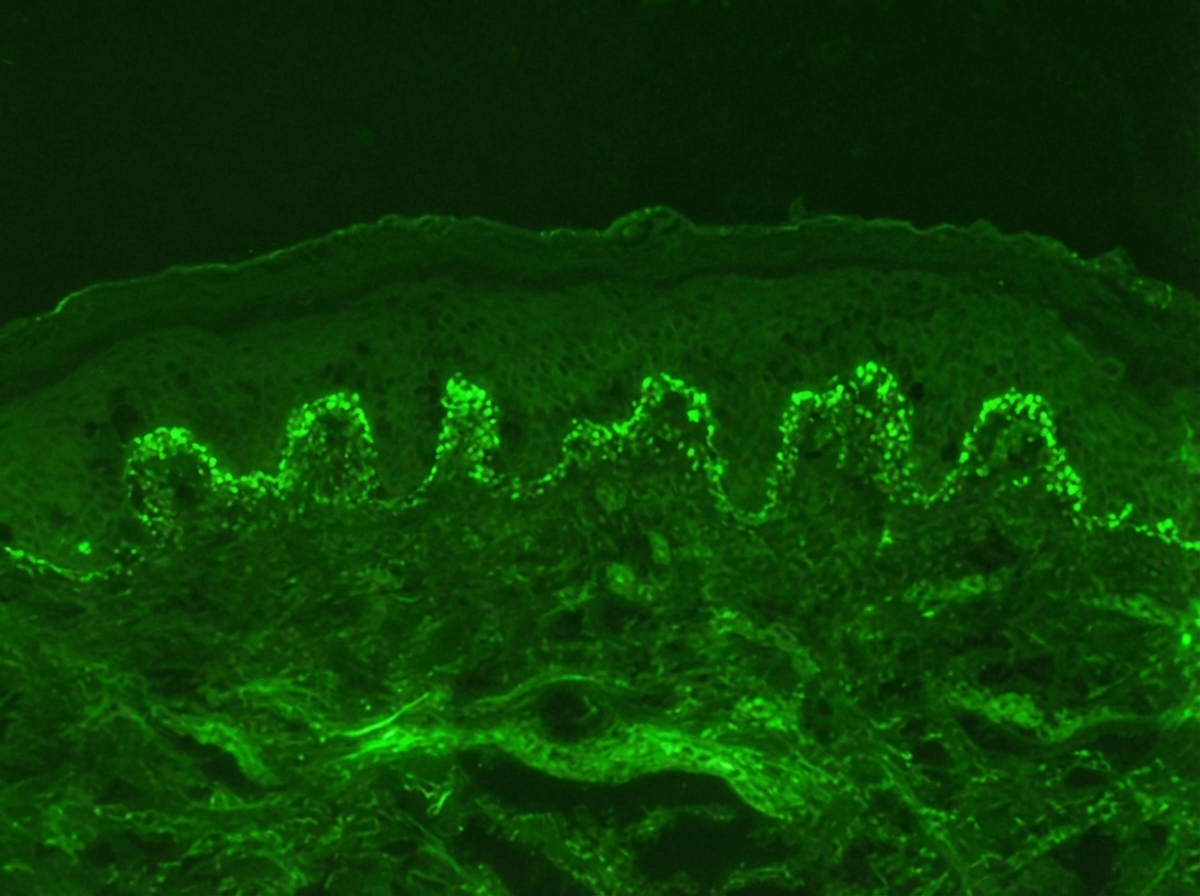
Identify the diagnosis based on the dermatology immunofluorescence (IF) image provided.
A 25-year-old patient presents with chronic itchy, erythematous skin lesions on the flexural areas that have been recurring since childhood. The patient has a family history of asthma. Which of the following is the most important diagnostic criterion for the most likely diagnosis?
"Isomorphic response" can be a feature of the following except
Which of the following is NOT a feature of atopic dermatitis?
The following lesion appears on the leg of a patient of ulcerative colitis. All are useful in management except:

Patient on anti-TB drugs develops tender nodules on shins. Most likely diagnosis is:
Most common precipitant of contact dermatitis is?
Identify the lesion: (Recent NEET Pattern 2016-17)

Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app