
Photoaging — MCQs

Chemical peeling is indicated in all of the following except
A patient consults a dermatologist about a skin lesion on her neck. Examination reveals a 1-cm diameter, red, scaly plaque with a rough texture and irregular margins. Biopsy demonstrates epidermal cells with large, pleomorphic, hyperchromatic nuclei. What is the most likely diagnosis?
Methoxysalen is used as:
Exposure to sunlight can precipitate chronic disc-shaped skin lesions characteristic of which of the following conditions?
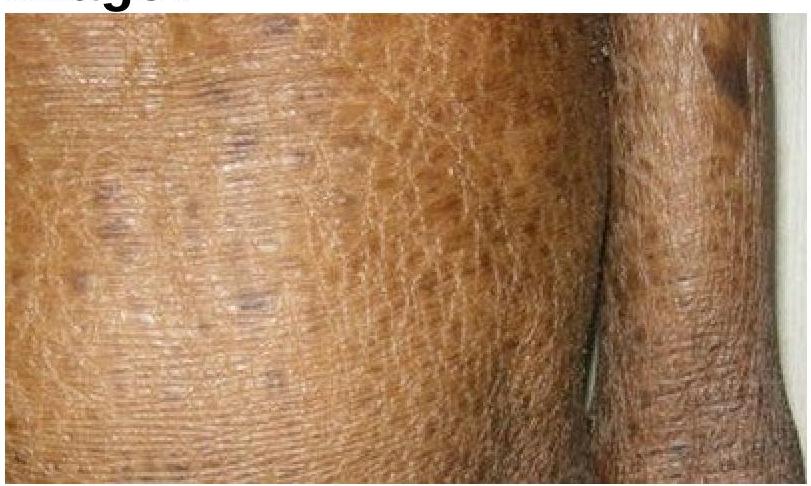
Identify the skin condition depicted in the image.
Which of the following statements is not correct regarding sebaceous cyst?
A cosmetic dermatologist plans to introduce microneedling radiofrequency for acne scars. Which parameter combination would provide optimal collagen remodeling with minimal risk of thermal injury in Fitzpatrick type IV skin?
A patient treated with Q-switched Nd:YAG laser for nevus of Ota develops paradoxical darkening after 4 weeks. What is the most likely explanation for this phenomenon?
A 42-year-old woman develops sudden onset vision loss in one eye 2 hours after hyaluronic acid filler injection in the glabella. Fundoscopy shows retinal whitening. What is the underlying pathophysiology?
A 28-year-old patient undergoes 70% glycolic acid peel for acne scars. Two hours post-procedure, he develops severe burning and erythema. What is the most appropriate immediate management?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app