
Basic Dermatology — MCQs

On this page
Where does nevus simplex commonly present?
A known case of diabetes develops annular orange skin lesions that disappear after a biopsy. What is the term used to describe this phenomenon?
What is the typical duration for pityriasis rosea to resolve?
Sebaceous cysts can occur in all the following locations in the body except:
1 to 2 mm haemorrhages in skin are known as:
Which glands are primarily affected by Fox Fordyce Disease?
Which skin condition is characterized by a 'Christmas tree' appearance?
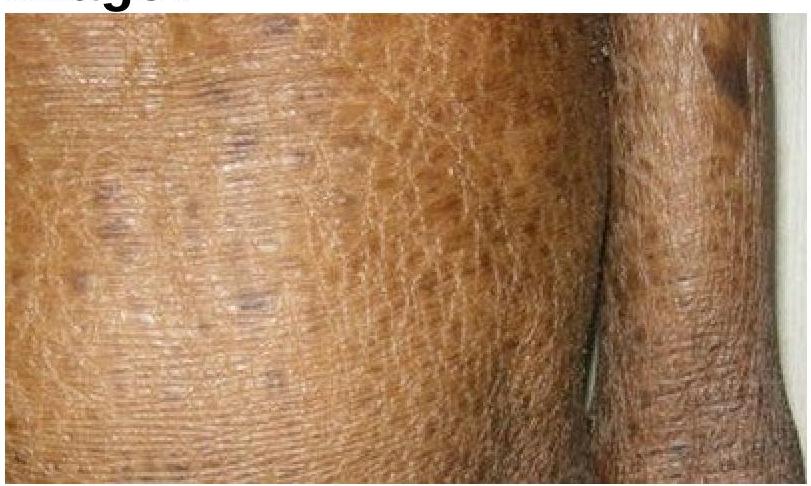
Identify the skin condition depicted in the image.
Which of the following statements is true regarding Acanthosis Nigricans?
Cutis marmorata occurs due to exposure to –
Practice by Chapter
Structure and Function of Skin
Practice Questions
Cutaneous Histopathology
Practice Questions
Dermatological Examination
Practice Questions
Skin Lesions: Morphology and Description
Practice Questions
Principles of Diagnosis in Dermatology
Practice Questions
Dermatological Procedures
Practice Questions
Wound Healing
Practice Questions
Cutaneous Immunology
Practice Questions
Genetics in Dermatology
Practice Questions
Cutaneous Manifestations of Systemic Diseases
Practice Questions
Geriatric Dermatology
Practice Questions
Pediatric Dermatology Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app