
Basic Dermatology — MCQs

On this page
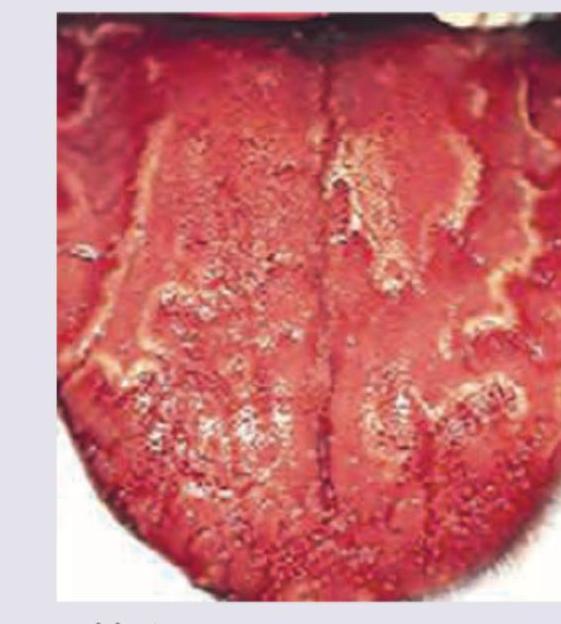
Identify the lesion seen on the tongue in the given image.
A 40 year old man with a known case of chronic pancreatitis presents to the OPD with complaint of skin pigmentation over the abdomen. The patient gives a history of chronic use of a hot water bottle to relieve the abdominal discomfort. Which one of the following is the most appropriate diagnosis?
A patient presents with orange-hued skin lesions and hyperkeratotic palms and soles. A biopsy shows alternating parakeratosis and orthokeratosis. What is the most likely diagnosis?
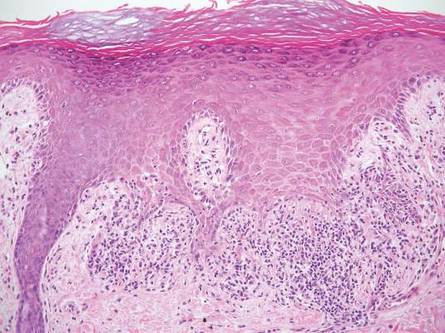
A patient's skin biopsy shows a box-shaped or square-shaped pattern of inflammatory infiltrate, as shown in the image. What is the most likely diagnosis?
A patient who has always neglected his nutrition presented with follicular hyperkeratosis on the extensor aspect of the forearm. What is the diagnosis?
A young girl presents to the outpatient department with rough-surfaced lesions over her elbows and knees. She also complains of diminished vision at night. What is the most likely diagnosis?
Match the following scale types with their lesions. | Scales | Lesions | | :-- | :-- | | 1. Collarette scales | a. Pityriasis versicolour | | 2. Silvery scales | b. Pityriasis rosea | | 3. Mica-like scales | c. Psoriasis | | 4. Branny scales | d. Pityriasis lichenoides |
A 24-year-old male presents with asymptomatic scaly lesions over the body as shown in the image below. What is the likely diagnosis?

Match the following woods lamp findings: 1. Erythrasma, 2. Pityriasis versicolor, 3. Tinea capitis, 4. Vitiligo || a. Yellow b. Coral red fluorescence c. Pink d. Green e. Milky white
A 30-year-old woman presents with multiple itchy, red patches on her body that have been present for several months. She reports that the lesions started on her chest and spread to other areas. Examination reveals multiple round-to-oval erythematous patches with fine scale. A KOH preparation is negative. Wood's lamp examination shows no fluorescence. Which of the following is the most likely diagnosis?
Practice by Chapter
Structure and Function of Skin
Practice Questions
Cutaneous Histopathology
Practice Questions
Dermatological Examination
Practice Questions
Skin Lesions: Morphology and Description
Practice Questions
Principles of Diagnosis in Dermatology
Practice Questions
Dermatological Procedures
Practice Questions
Wound Healing
Practice Questions
Cutaneous Immunology
Practice Questions
Genetics in Dermatology
Practice Questions
Cutaneous Manifestations of Systemic Diseases
Practice Questions
Geriatric Dermatology
Practice Questions
Pediatric Dermatology Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app