
Basic Dermatology — MCQs

On this page
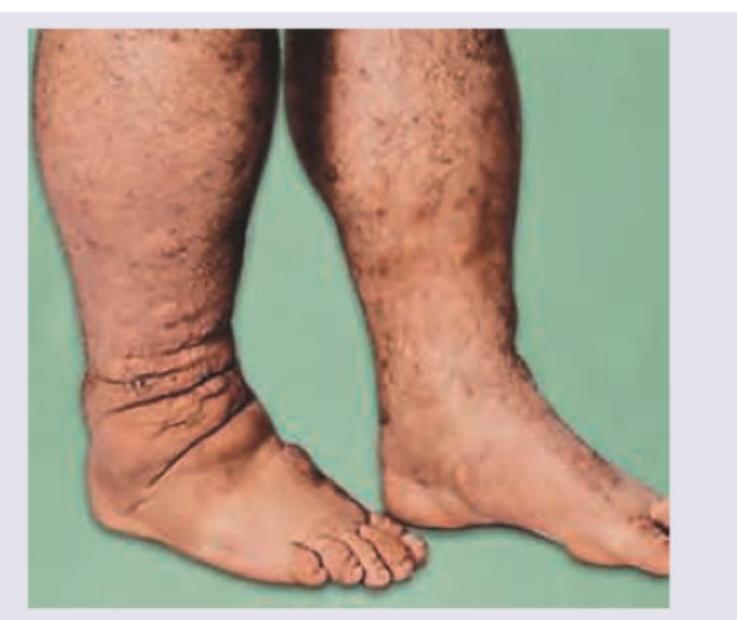
All are reported triggers or associations of the skin lesion shown except:

Pseudo Nikolsky sign is seen in all except:
The following skin condition is associated with:

The skin condition shown in the image is associated with?
The following image shows:

The following image shows:
The image shows a child with?

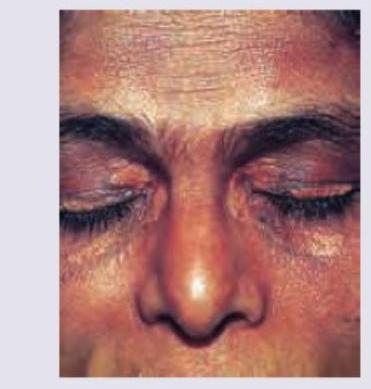
A 30-year-old woman presents with a cosmetic complaint shown in the image. What is the clinical diagnosis?
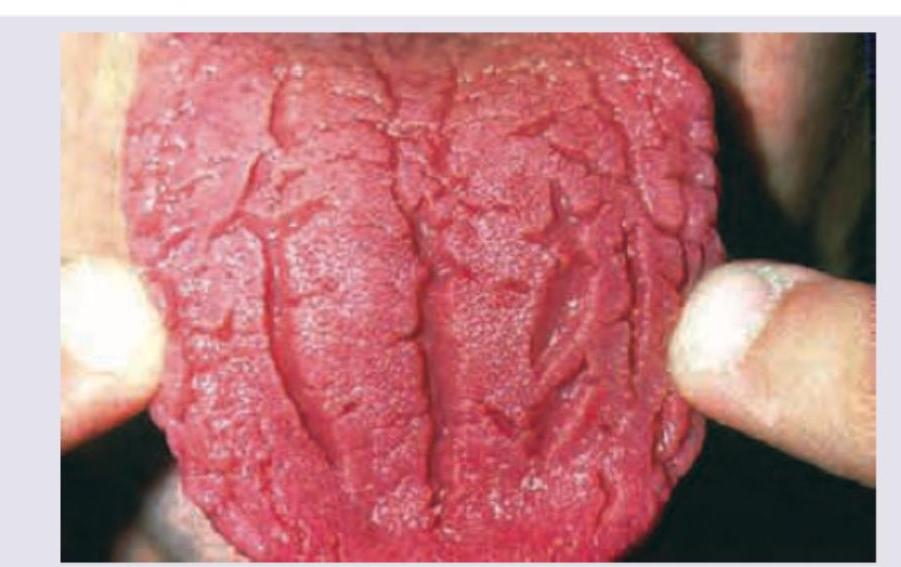
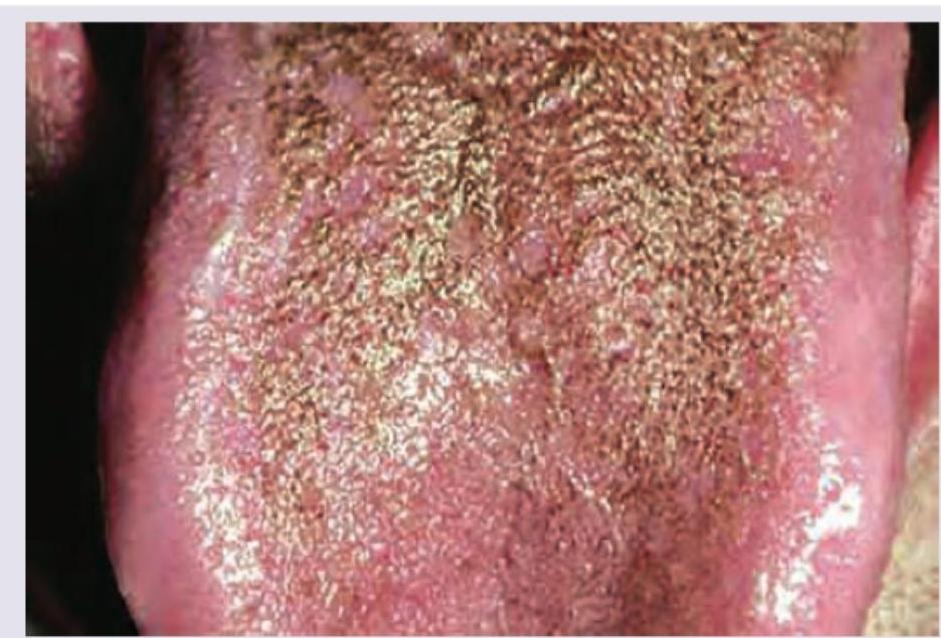
All are causes of following tongue appearance except: (Recent NEET Pattem 2016-17)
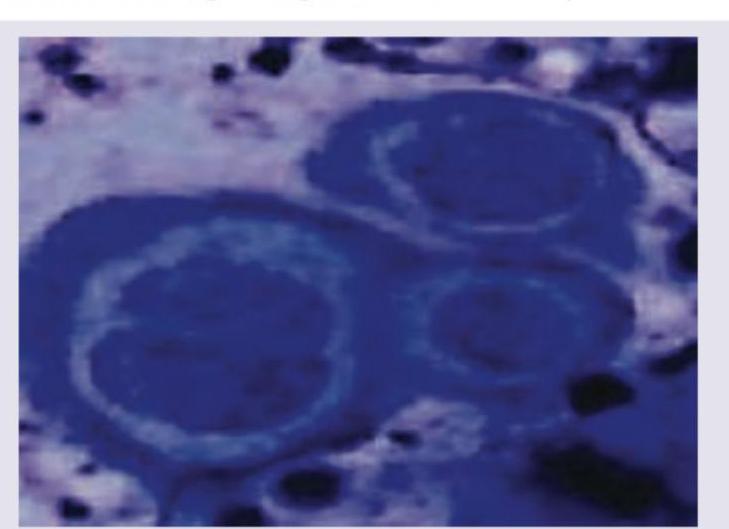
The image shows presence of:
Practice by Chapter
Structure and Function of Skin
Practice Questions
Cutaneous Histopathology
Practice Questions
Dermatological Examination
Practice Questions
Skin Lesions: Morphology and Description
Practice Questions
Principles of Diagnosis in Dermatology
Practice Questions
Dermatological Procedures
Practice Questions
Wound Healing
Practice Questions
Cutaneous Immunology
Practice Questions
Genetics in Dermatology
Practice Questions
Cutaneous Manifestations of Systemic Diseases
Practice Questions
Geriatric Dermatology
Practice Questions
Pediatric Dermatology Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app