
Basic Dermatology — MCQs

On this page
Identify the lesion: (Recent NEET Pattern 2016-17)

A patient presents with acute, tender, non-ulcerating nodules over the anterior shins for the past 2 weeks. These lesions are seen in which of the following?

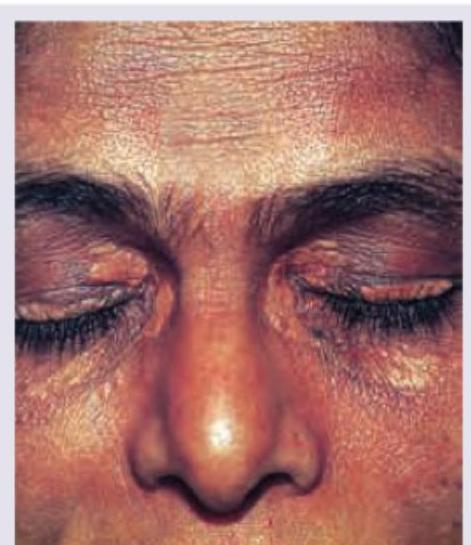
A 65-year-old patient presents with development of multiple papules and nodules around the right knee for last one year. Which of the following hyper-lipoproteinemia is associated with this condition?

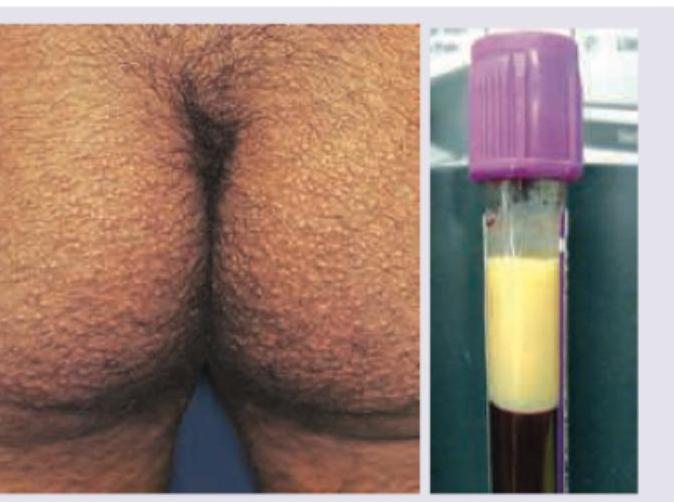
A 55-year-old patient presented with following lesions on his buttock. He consulted a general physician who diagnosed it as an allergy, but lesions are persisting. His blood sample was drawn and shows a creamy top layer. What is the diagnosis?
The following skin lesion can be seen in all except:
A 26-year-old male presents with greasy papules on face and chest that feel like sandpaper. Palms and soles have minute pits. Skin biopsy was performed. What is the diagnosis?
This is the clinical presentation of a 5-year-old boy with lesions worsening in cold weather. His mother says these lesions developed after 1 year of age. His sister has same lesions which developed after 2 years of age. All are true about the condition except:

All are true about the lesion shown except:

Identify which of the following tests is being done?

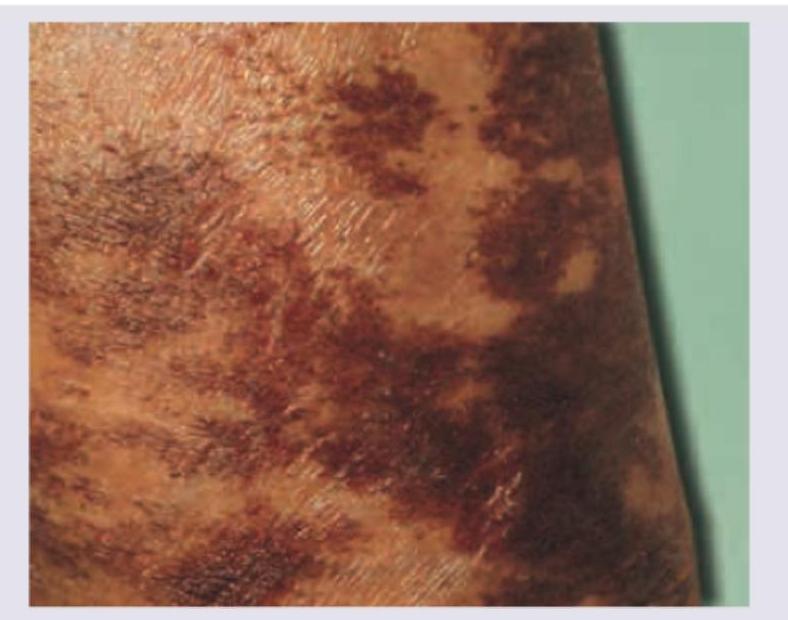
A patient with pancreatic tumor and impaired glucose tolerance is having these lesions on flexural areas. What is the diagnosis?
Practice by Chapter
Structure and Function of Skin
Practice Questions
Cutaneous Histopathology
Practice Questions
Dermatological Examination
Practice Questions
Skin Lesions: Morphology and Description
Practice Questions
Principles of Diagnosis in Dermatology
Practice Questions
Dermatological Procedures
Practice Questions
Wound Healing
Practice Questions
Cutaneous Immunology
Practice Questions
Genetics in Dermatology
Practice Questions
Cutaneous Manifestations of Systemic Diseases
Practice Questions
Geriatric Dermatology
Practice Questions
Pediatric Dermatology Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app