
Basic Dermatology — MCQs

On this page
Which condition presents with 'Cayenne pepper' stippling due to hemosiderin?
A 26-year-old recently married woman presents with tender nodules on her shin. What is the most important initial history to obtain?
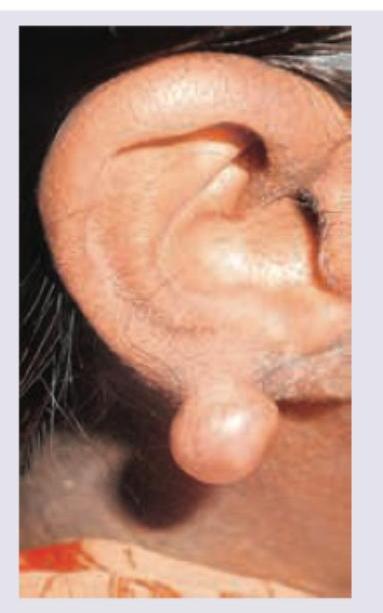
A 45-year-old patient with a history of elevated cholesterol levels presents with nodular swellings over the elbow. The lesion is a superficial, lobulated subcutaneous nodule over the olecranon that is not fixed to or continuous with the triceps tendon. The lesion shown in the image is most likely:

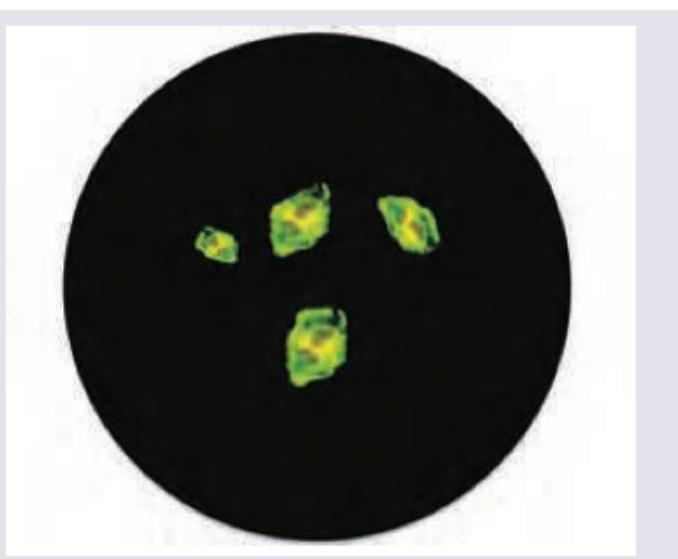
The following finding of acantholytic cells on Tzanck smear can be seen in:
The first line intralesional treatment for this condition is:
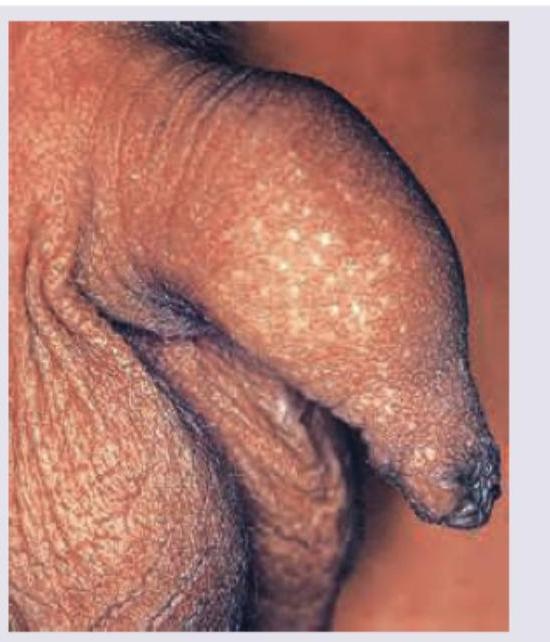
A 20-year-old male with no history of any sexual contact presents with following lesions on his penis. What is the diagnosis?
A 41-year-old male complains of itching on the upper chest for one month. He initially noticed a single large oval patch on his trunk, followed by multiple smaller oval lesions with collarette scale arranged along the skin cleavage lines. What is the most likely diagnosis?

Identify the lesion:

A 16-year-old boy with cryptorchidism presents with dry skin. Identify the lesion:

Identify the lesion: (Recent NEET Pattern 2016-17)

Practice by Chapter
Structure and Function of Skin
Practice Questions
Cutaneous Histopathology
Practice Questions
Dermatological Examination
Practice Questions
Skin Lesions: Morphology and Description
Practice Questions
Principles of Diagnosis in Dermatology
Practice Questions
Dermatological Procedures
Practice Questions
Wound Healing
Practice Questions
Cutaneous Immunology
Practice Questions
Genetics in Dermatology
Practice Questions
Cutaneous Manifestations of Systemic Diseases
Practice Questions
Geriatric Dermatology
Practice Questions
Pediatric Dermatology Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app