
Geriatric Dermatology — MCQs

A 40 year old woman presents with a 2 year history of erythematous papulopustular lesions on convexities of the face. There is a background of erythema & telangiectasia. The most likely diagnosis is –
Actinic keratoses are associated with
A 60-year-old female presents with eczematous itching lesions. Biopsy revealed a subepidermal cleft with Direct Immunofluorescence showing Linear C3 & IgG deposition along the basement membrane zone. What is the likely diagnosis?
A patient presents with a skin rash that is exaggerated on sun exposure. What is the repair mechanism involved in this condition?
A 25-year-old male presents with a cluster of vesicles along the dermatome on his chest and back. He complains of burning pain in the same area. What is the most likely diagnosis?
A male patient presented with a 0.3 cm nodule on the left nasolabial fold. A pathological examination revealed a basaloid appearance with peripheral palisading. What is the most likely diagnosis?

A patient presents with the skin lesions shown in the image. While evaluating for possible blistering disorders, all of the following conditions could present with similar morphology EXCEPT:

Which of the following is the MOST characteristic feature of skin tags (acrochordons)?
During tattooing, in which layer of the skin is the pigment/ink primarily deposited?
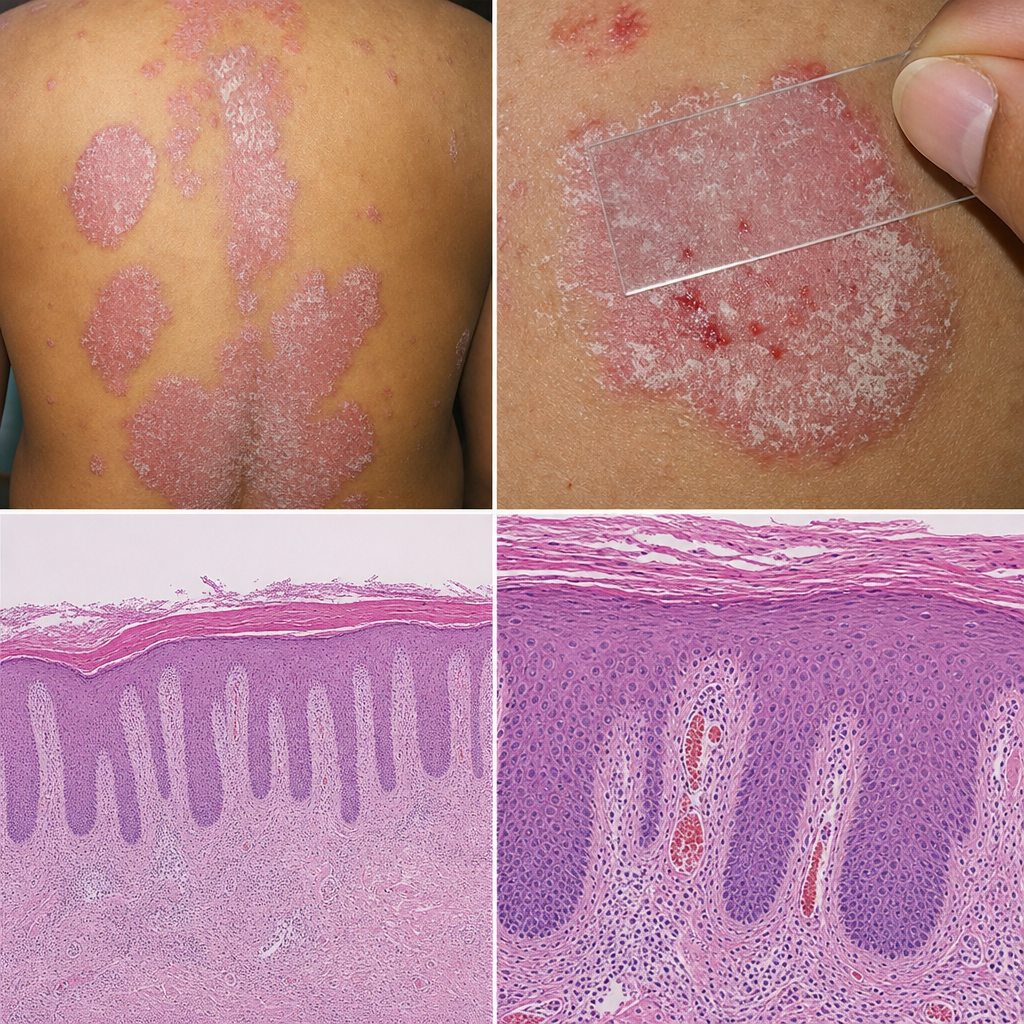
A 35-year-old man presents with a 2-year history of recurring itchy skin lesions that worsen in winter. His father had a similar condition. Examination reveals Auspitz sign on gentle scraping. The skin findings are shown in Image 1. Which of the following pathophysiological mechanisms is most directly responsible for the sign elicited on scraping in this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app