
Dermatological Examination — MCQs

Identify the skin lesion shown in the image.

Diascopy is very helpful in the diagnosis of:
A child has a rash. His family history is positive for asthma. What could be the most probable diagnosis?

A 30-year-old male presented with silvery scales on elbow and knee, that bleed on removal. The probable diagnosis is:
Koebner's phenomenon seen in ?
Which of the following methods is used for demonstrating old washed bloodstains?
A farmer presented with a black mole on the cheek. It increased in size, more than 6mm with irregular borders and a central black lesion, what could be the diagnosis?
Dyskeratosis refers to which of the following?
What is the optimal wavelength of light emitted by a Wood's lamp for dermatological examinations?
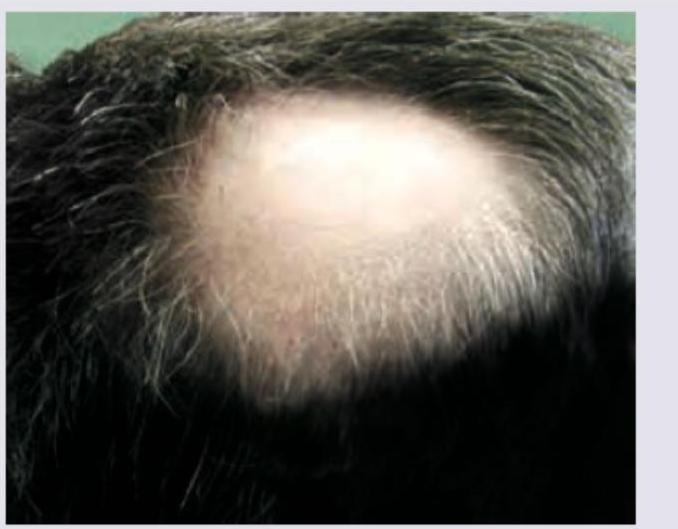
In a patient with the following lesion on scalp, what changes are seen in the nails?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app