
Cutaneous Immunology — MCQs

What is the primary function of Langerhans' cells?
A 32 year old man presents with a 3-month history of weight loss, night sweats, a productive cough with blood-tinged sputum, anorexia, general malaise, and a low grade fever. A PPD skin test shows > 10 mm of induration. If the area of induration were biopsied, which of the following type of reactive cells would be found?
A 60-year-old female presents with eczematous itching lesions. Biopsy revealed a subepidermal cleft with Direct Immunofluorescence showing Linear C3 & IgG deposition along the basement membrane zone. What is the likely diagnosis?
Statement 1 - A 59-year-old patient presents with flaccid bullae. Histopathology shows a suprabasal acantholytic split. Statement 2 - The row of tombstones appearance is diagnostic of Pemphigus vulgaris.
Most common precipitant of contact dermatitis is?
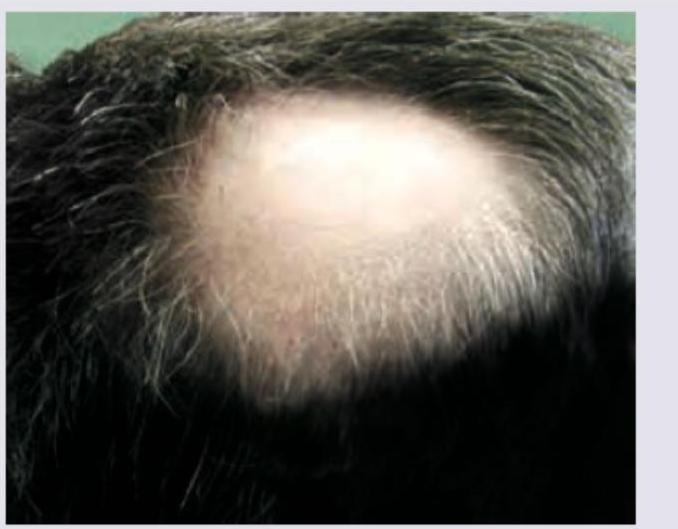
In a patient with the following lesion on scalp, what changes are seen in the nails?
In which of the following conditions is the Koebner phenomenon most commonly observed?
Patient on anti-TB drugs develops tender nodules on shins. Most likely diagnosis is:
Lines of Blaschko are related to?
During tattooing, in which layer of the skin is the pigment/ink primarily deposited?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app