
Basic Dermatology — MCQs

On this page
During tattooing, in which layer of the skin is the pigment/ink primarily deposited?
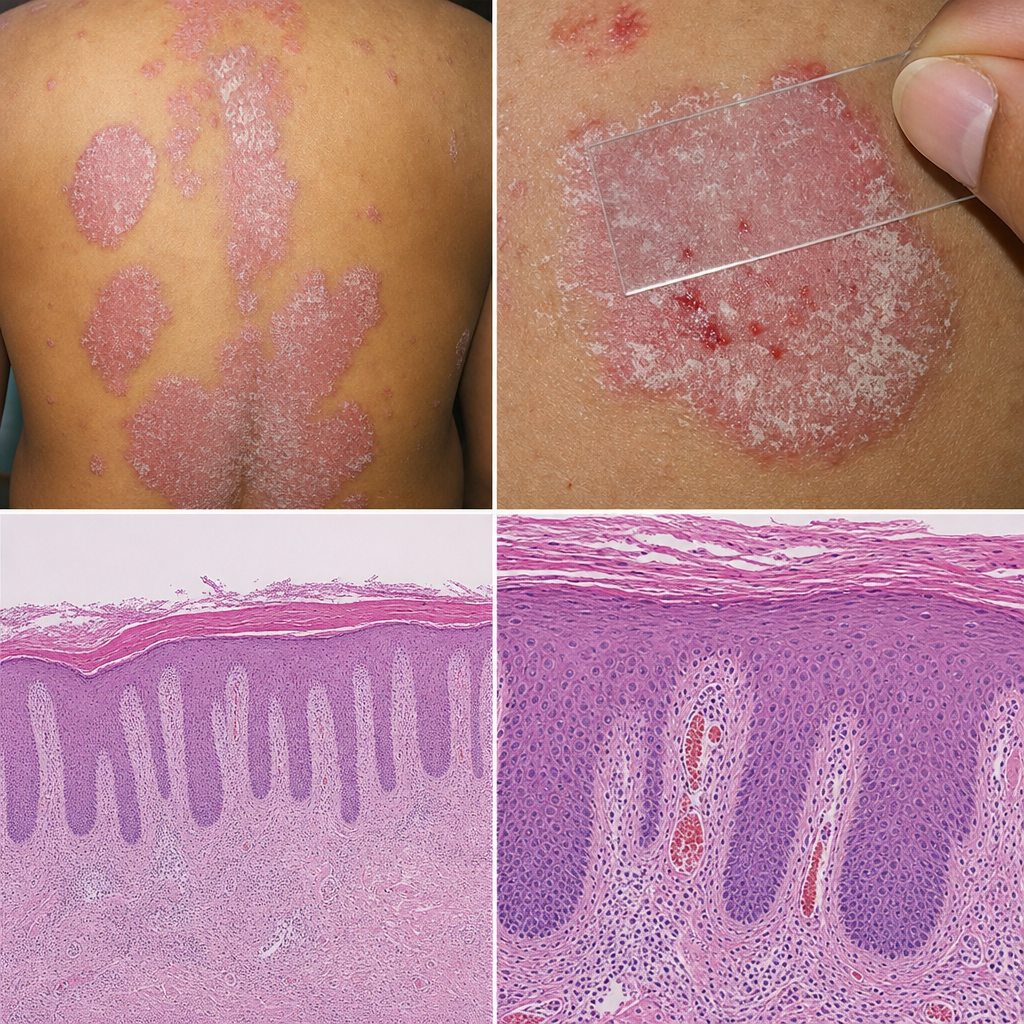
A 35-year-old man presents with a 2-year history of recurring itchy skin lesions that worsen in winter. His father had a similar condition. Examination reveals Auspitz sign on gentle scraping. The skin findings are shown in Image 1. Which of the following pathophysiological mechanisms is most directly responsible for the sign elicited on scraping in this patient?
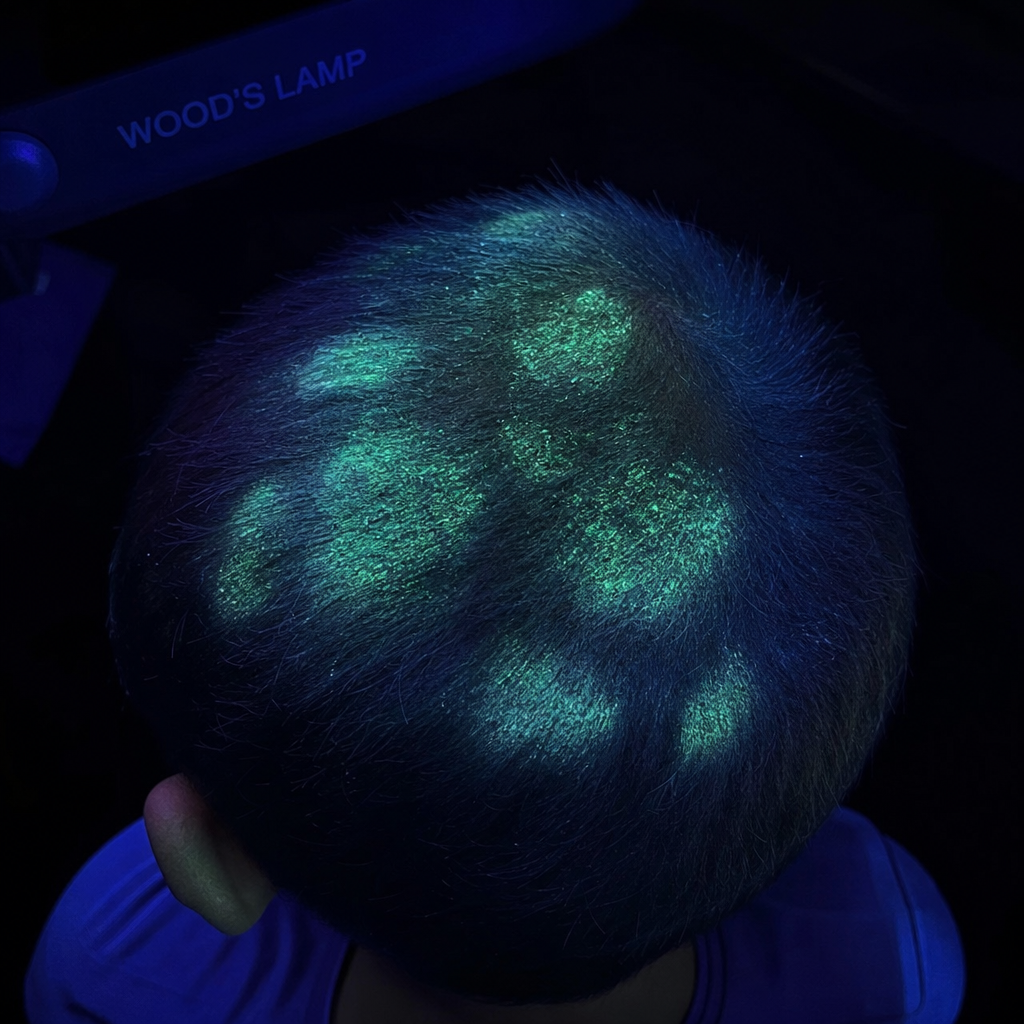
A 9-year-old boy is brought with a 3-week history of patchy hair loss on the scalp associated with mild scaling and broken hair stubs. Several classmates have similar complaints. The school nurse noted the lesions fluoresce under a special lamp. The Wood's lamp examination is shown (Image 1). Which of the following is the most appropriate treatment for this condition?
Which Fitzpatrick skin type is most prone to post-inflammatory hyperpigmentation after laser therapy?
A young female presents with a history of fever and a nodular lesion over the shin. Histopathology reveals foamy histiocytes with neutrophilic infiltration. There is no evidence of vasculitis. What is the most probable diagnosis?
What is the primary lesion in lichen planus?
A 22-year-old female presents with dry papules in the seborrheic areas, especially in the summer. Her father also has a history of similar lesions. What is the most probable diagnosis?
A 16-year-old boy presented with asymptomatic, multiple erythematous annular lesions with a collarette of scales at the periphery of the lesions present on the trunk. What is the most likely diagnosis?
Which of the following is not a type of leukoplakia?
Facial edema, cheilitis granulomatosa, and a fissured tongue characterize which of the following syndromes?
Practice by Chapter
Structure and Function of Skin
Practice Questions
Cutaneous Histopathology
Practice Questions
Dermatological Examination
Practice Questions
Skin Lesions: Morphology and Description
Practice Questions
Principles of Diagnosis in Dermatology
Practice Questions
Dermatological Procedures
Practice Questions
Wound Healing
Practice Questions
Cutaneous Immunology
Practice Questions
Genetics in Dermatology
Practice Questions
Cutaneous Manifestations of Systemic Diseases
Practice Questions
Geriatric Dermatology
Practice Questions
Pediatric Dermatology Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app