
Diagnostic Methods in Autoimmune Dermatoses — MCQs

Best site for taking biopsy for HSV esophagitis is:
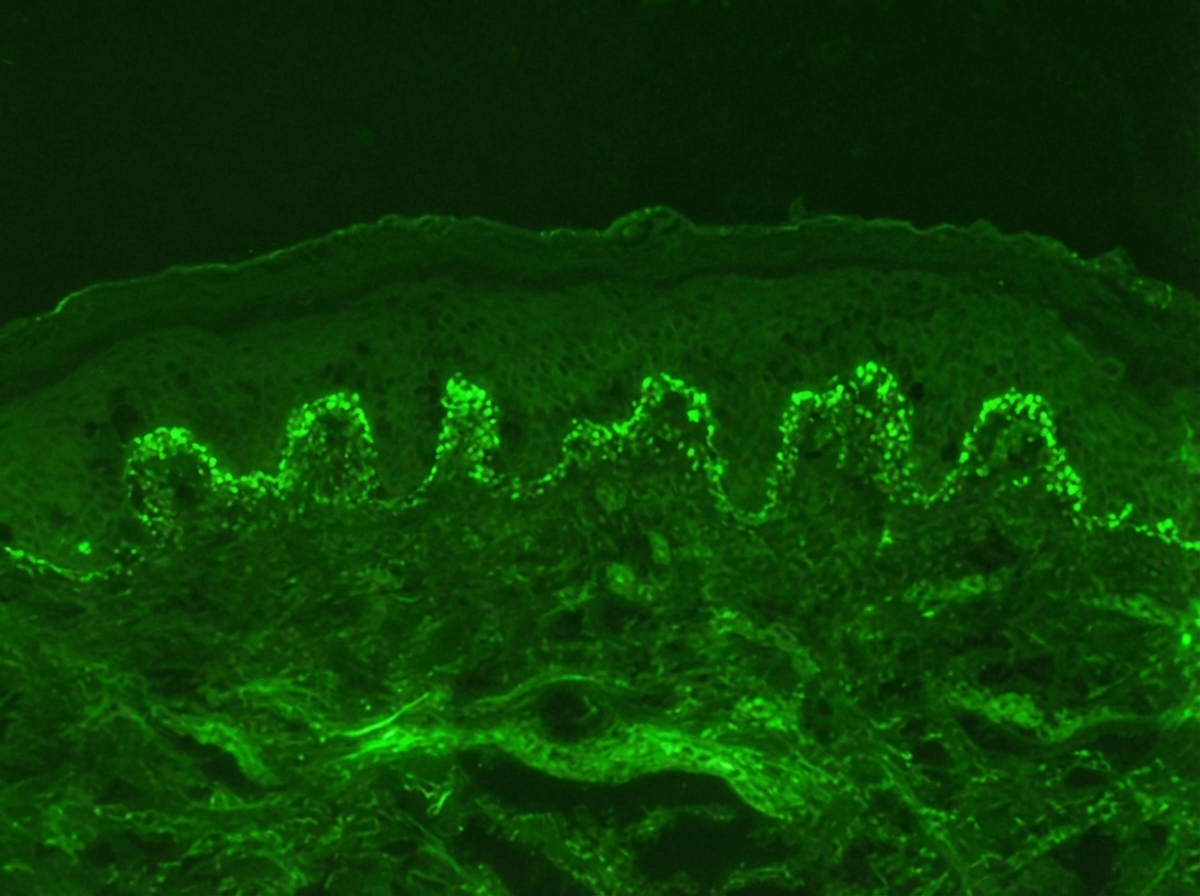
Identify the diagnosis based on the dermatology immunofluorescence (IF) image provided.
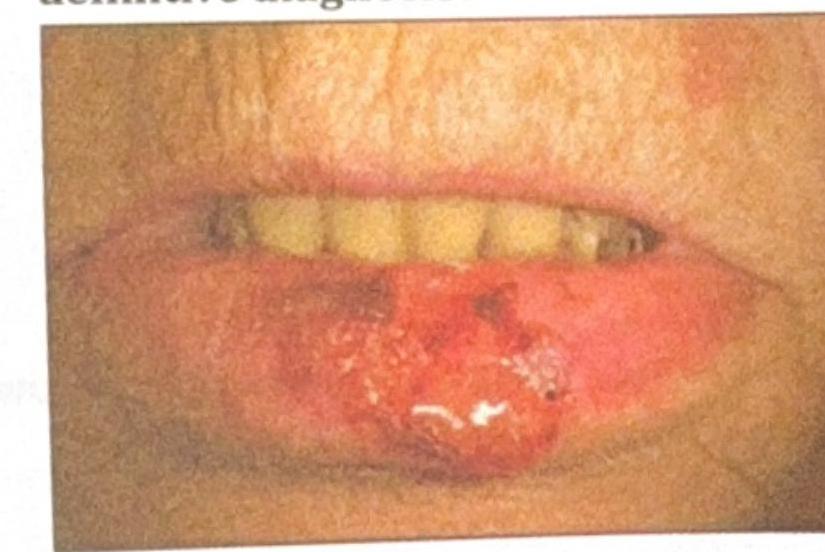
An elderly patient presents with a non-healing ulcerative lesion on the lower lip, as shown in the image. The lesion has been gradually enlarging over the past few months. Suspecting squamous cell carcinoma (SCC), what is the most appropriate method to obtain a biopsy for definitive diagnosis?
Acute febrile neutrophilic dermatosis is seen in-
Which of the following statements about actinic lichen planus is false?
Which of the following is a xenodiagnostic method?
A skin biopsy shows suprabasilar acantholysis with 'row of tombstones' appearance. Which immunofluorescence pattern would confirm pemphigus vulgaris?
A child was diagnosed as a case of pauci-immune crescentic glomerulonephritis. The treatment to be given in this child is –
Patient presenting with cutaneous vasculitis, glomerulonephritis, peripheral neuropathy, which investigation is to be performed next that will help you diagnose the condition?
All of the following are true for sympathetic ophthalmitis except which of the following?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app