
Acne and Related Disorders — MCQs

On this page
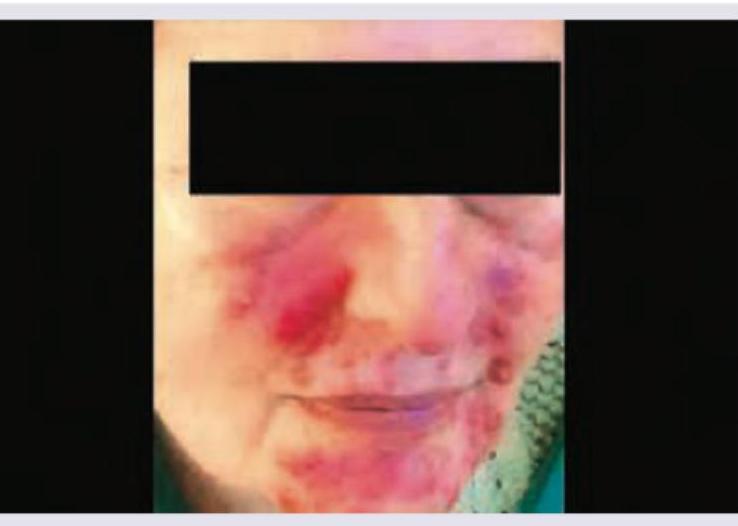
A 25-year-old girl presents with papules, erythema and telangiectasia over the face as shown below. She also gives a history of flushing and burning sensation on exposure to sun and on any emotional disturbance. The most likely diagnosis is? (AIIMS Nov 2016)
A young boy with oily skin presents with predominantly comedonal acne as shown. What is the preferred first-line monotherapy?

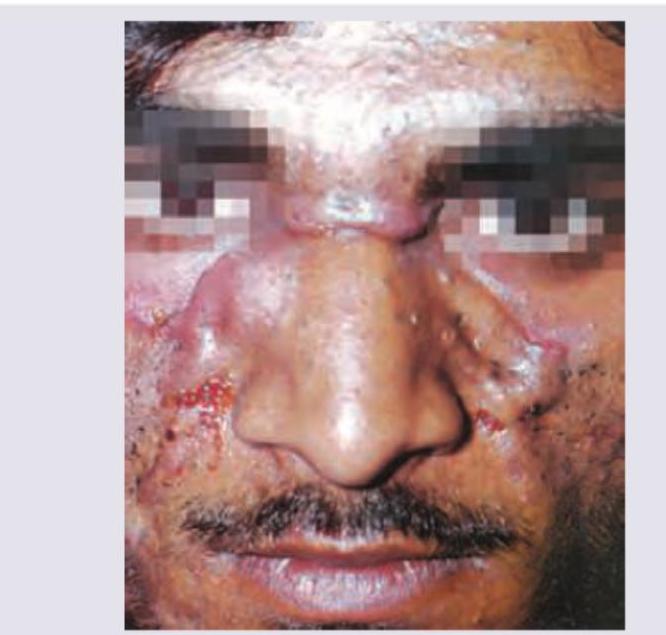
A 22-year-old male presents with a slowly progressive facial skin condition that has been worsening over the past 2 years. He reports no fever, joint pain, or systemic symptoms. Examination reveals numerous interconnected nodules, cysts, and communicating sinus tracts with extensive scarring. What does the given image show?

All are true about the condition shown in the figure except: (Recent NEET Pattern 2016-17)

The image is diagnostic of?
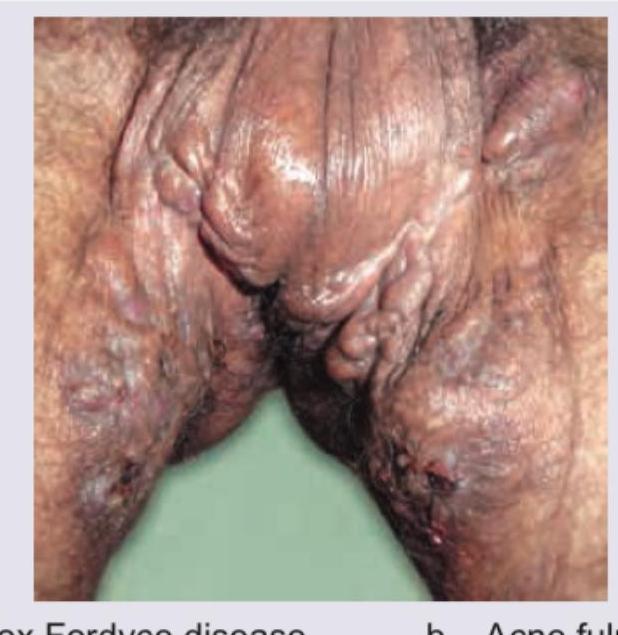
A 25-year-old female presents with the following lesions in the axilla, as shown by the arrow:

A young male smoker presents with long standing history of lesions in axilla. All are correct about the image shown below except:

A patient presents with 1-year history of painful nodulocystic acne as shown in the image. Which of the following is the drug of choice for this case?
An obese 45-year-old lady who is a chronic smoker came with tender subcutaneous nodules with chronic inflammation with scarring under her left axilla. She is likely to be suffering from:
Which of the following is the causative agent for acne fulminans?
Practice by Chapter
Acne Vulgaris: Pathophysiology
Practice Questions
Acne Vulgaris: Clinical Types
Practice Questions
Acne Vulgaris: Management
Practice Questions
Acne in Special Populations
Practice Questions
Rosacea
Practice Questions
Perioral Dermatitis
Practice Questions
Hidradenitis Suppurativa
Practice Questions
Acne Keloidalis Nuchae
Practice Questions
Acne Scarring and Its Management
Practice Questions
Psychological Aspects of Acne
Practice Questions
Diet and Acne
Practice Questions
Newer Therapies in Acne Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app