
Acne and Related Disorders — MCQs

On this page
A 72-year-old fair-skinned farmer presents with a slowly enlarging, non-healing lesion on his nose that occasionally bleeds. He reports decades of outdoor sun exposure. The lesion has been present for approximately 18 months. On examination, a pearly, translucent nodule with rolled telangiectatic borders and central ulceration is noted on the nasal ala — a high-risk H-zone location. Which of the following is the most appropriate primary treatment for this lesion?

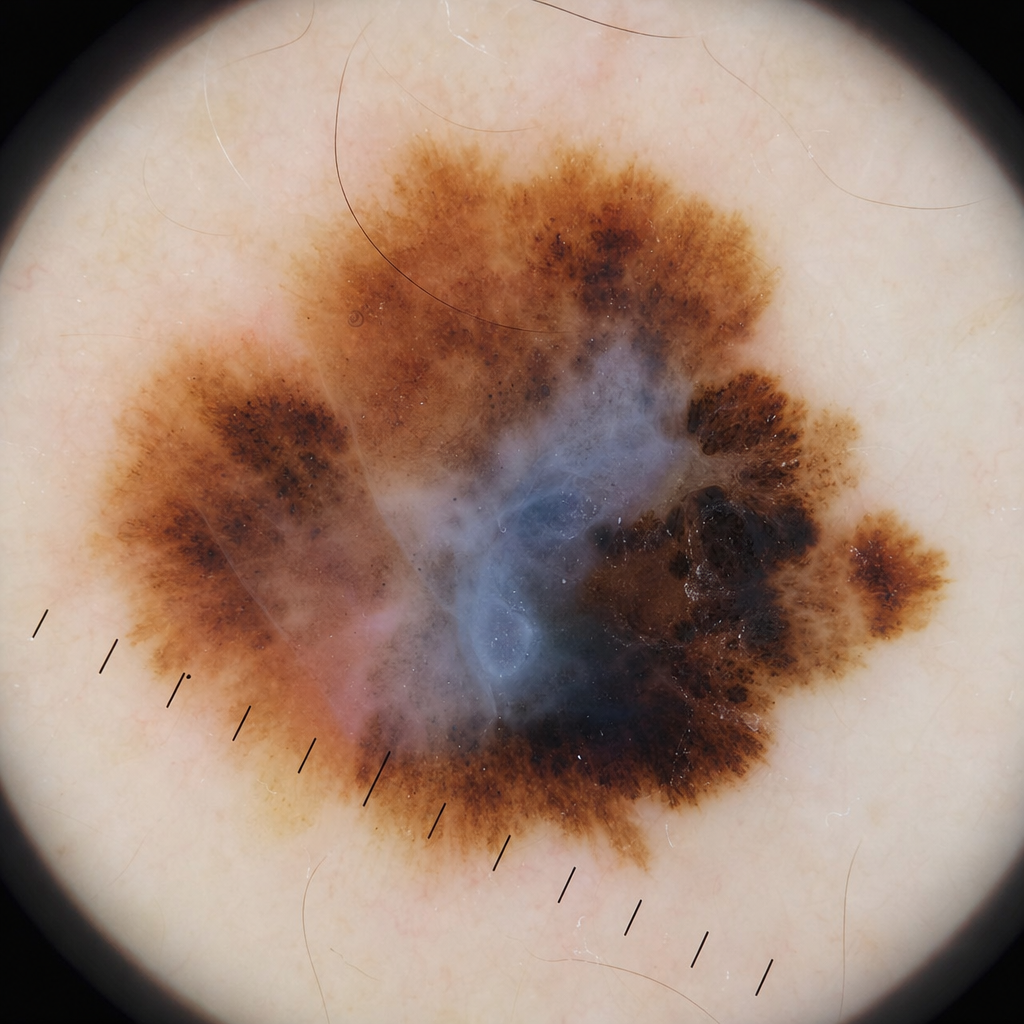
A 52-year-old fair-skinned man presents with a 1.2 cm pigmented lesion on his back that has changed in colour and border over the past 6 months. His GP referred him after noting asymmetry on clinical examination. The dermoscopy image is shown in (Image 1). Which of the following dermoscopic structures most specifically supports a diagnosis of malignancy in this lesion?
An 18-year-old girl presents with predominantly comedonal acne. What is the first-line treatment?
Which of the following drugs should not be used in the management of Rosacea?
Hypertrophy of the sebaceous glands in the nasal skin is called?
Which of the following is the main etiological factor for Hidradenitis suppurativa?
What is the most common site for Necrobiosis Lipoidica Diabeticorum?
A patient presented with the following symptoms. What is the etiopathogenesis of the disease process?

The condition seen in the illustration is:

A patient presented with multiple nodulocystic lesions on the face. Which is the drug of choice for this condition?
Practice by Chapter
Acne Vulgaris: Pathophysiology
Practice Questions
Acne Vulgaris: Clinical Types
Practice Questions
Acne Vulgaris: Management
Practice Questions
Acne in Special Populations
Practice Questions
Rosacea
Practice Questions
Perioral Dermatitis
Practice Questions
Hidradenitis Suppurativa
Practice Questions
Acne Keloidalis Nuchae
Practice Questions
Acne Scarring and Its Management
Practice Questions
Psychological Aspects of Acne
Practice Questions
Diet and Acne
Practice Questions
Newer Therapies in Acne Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app