
Social and Behavioral Sciences — MCQs

On this page
Acculturation may take place by what means?
Arrange the following stages of the family life cycle in chronological sequence?
Who proposed the concept of negative reinforcement?
Which of the following is an example of disability limitation?
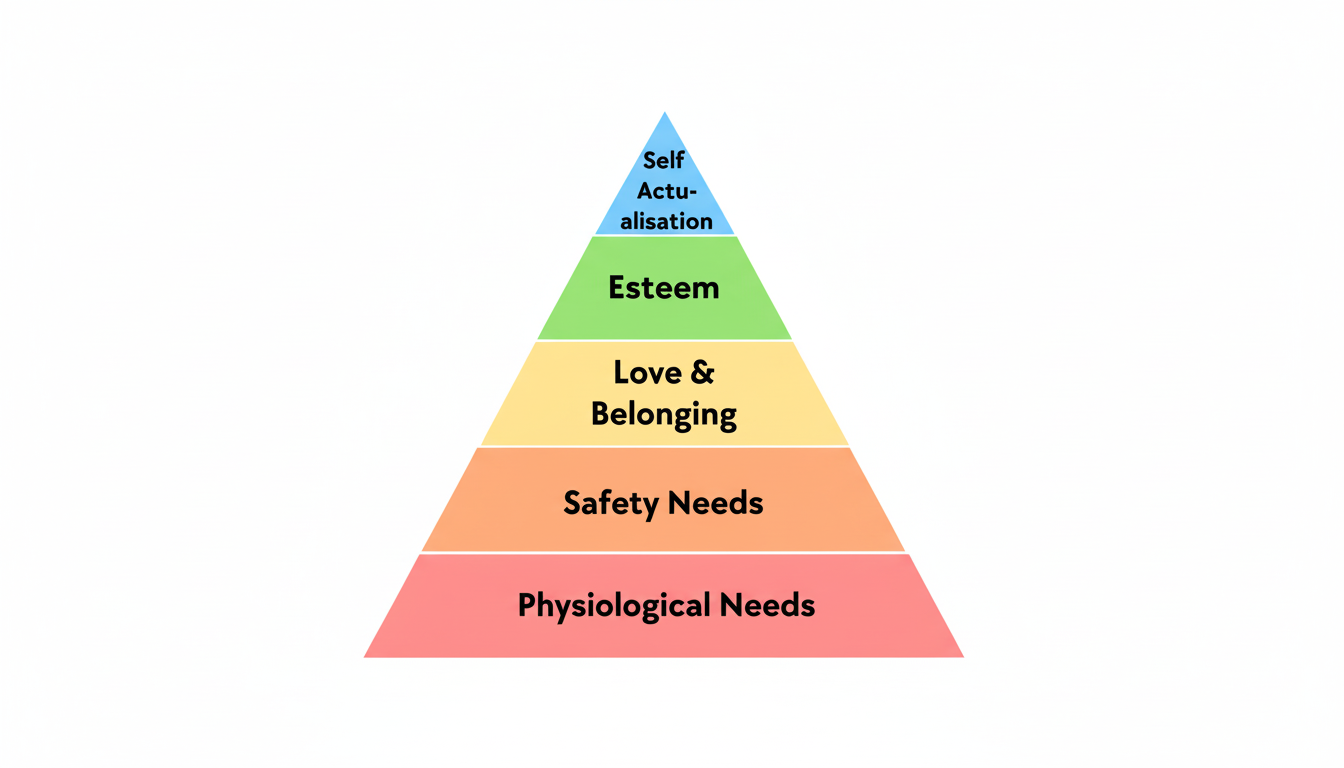
According to Maslow's hierarchy of needs, which level is at the top of the pyramid?
What is the name of the following pyramid?
Who first introduced the concept of Social Medicine?
Which of the following is NOT a scale used to measure socio-economic status?
Which of the following represents a non-deliberate cultural practice leading to an anti-mosquito effect?
All of the following are parts of cognitive behavior change techniques except?
Practice by Chapter
Social Determinants of Health
Practice Questions
Health Behavior Models
Practice Questions
Health Promotion
Practice Questions
Behavior Change Communication
Practice Questions
Cultural Aspects of Health
Practice Questions
Social Stigma and Health
Practice Questions
Gender and Health
Practice Questions
Social Support and Health
Practice Questions
Community Participation
Practice Questions
Qualitative Research Methods
Practice Questions
Health Psychology
Practice Questions
Social Marketing in Health
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app