
Occupational Health — MCQs

On this page
Under the Employees' State Insurance Act 1948, if the sickness of an insured person is duly certified by an Insurance Medical Officer, periodical cash payment benefit is payable for a maximum period of how many days in any continuous period of 365 days, as Sickness Benefit?
Vibration white finger refers to :
The Employees State Insurance Act, 1948 of India provides for certain benefits to employees. Which among the following are benefits to insured persons or to other dependents under the Act ? 1. Disablement benefit 2. Funeral expenses 3. Maternity benefit 4. Travel benefit Select the correct answer using the code given below :
Exposure to gases is a common hazard in industries. The gases can be classified as simple asphyxiants, chemical asphyxiants and anaesthetic gases. Which among the following are chemical asphyxiating gases ? 1. Carbon monoxide 2. Chloroform 3. Cyanide gas 4. Hydrogen Select the correct answer using the code given below :
With regard to lead poisoning, consider the following statements : 1. Coproporphyrin in urine is a useful screening test. 2. Hand washing before eating is an important measure of personal hygiene. 3. The use of d-penicillamine has been reported to be effective in management. How many of the statements given above is/are correct ?
With reference to occupational cancers, consider the following statements : 1. Skin cancer is a common occupational hazard in workers employed in nickel and chromium work. 2. Cancer bladder is an occupational hazard in workers employed in dye-stuffs and dyeing industry. 3. Leukaemia can occur on long exposure to benzol. 4. Lung cancer is typically found in workers employed in electric cable industries. Which of the statements given above are correct ?
Raju is 30 years of age. He has been working in the ceramic and pottery industry for the last 10 years. Which one of the following conditions should he be screened for?
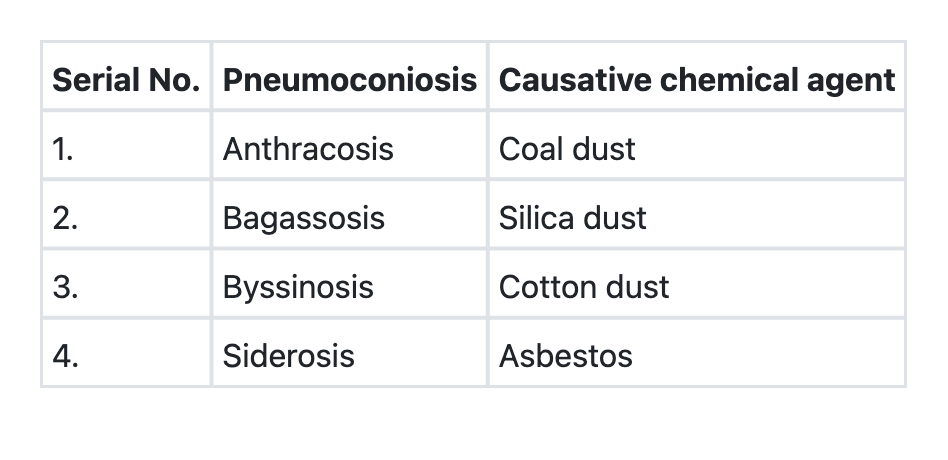
The following table shows some of the pneumoconioses diseases along with the most implicated causative chemical agents. Which among the following represent the correct combinations of diseases and causative chemical agents? Select the correct answer using the code given below.
Basophilic stippling of the RBCs is a sensitive index of
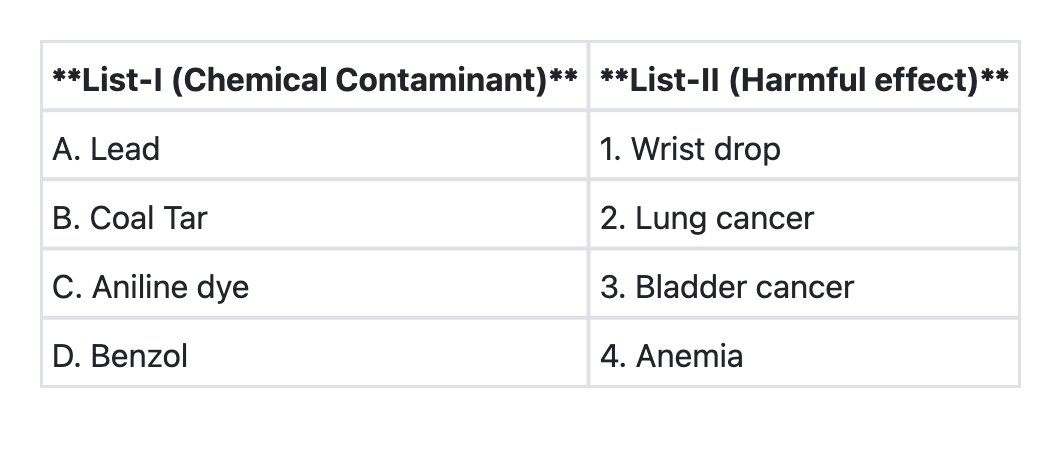
Match List-I with List-II and select the correct answer using the code given below the Lists:
Practice by Chapter
Occupational Hazards: Classification
Practice Questions
Occupational Diseases
Practice Questions
Ergonomics
Practice Questions
Industrial Toxicology
Practice Questions
Occupational Cancers
Practice Questions
Work-Related Musculoskeletal Disorders
Practice Questions
Occupational Health Services
Practice Questions
Industrial Hygiene
Practice Questions
Assessment of Work Environment
Practice Questions
Personal Protective Equipment
Practice Questions
Occupational Health Legislation
Practice Questions
Workers' Compensation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app