
Protein-Energy Malnutrition — MCQs

A 5-year-old has the following anthropometry findings: Weight/age < -3.2 SD, Height/age < -2.5 SD, Weight/height < -1.7 SD. What is the most likely diagnosis?
Which of the following anthropometric indicators best reflects acute malnutrition (wasting) in children?
Which of the following is NOT a symptom of Kwashiorkor?
Which is the most specific clinical feature for diagnosis of Kwashiorkor?
Kwashiorkor is diagnosed in growth-retarded children along with:
Retardation of skeletal maturity can be caused by all of the following except:
Which of the following anthropometric indicators best reflects acute malnutrition (wasting) in children?
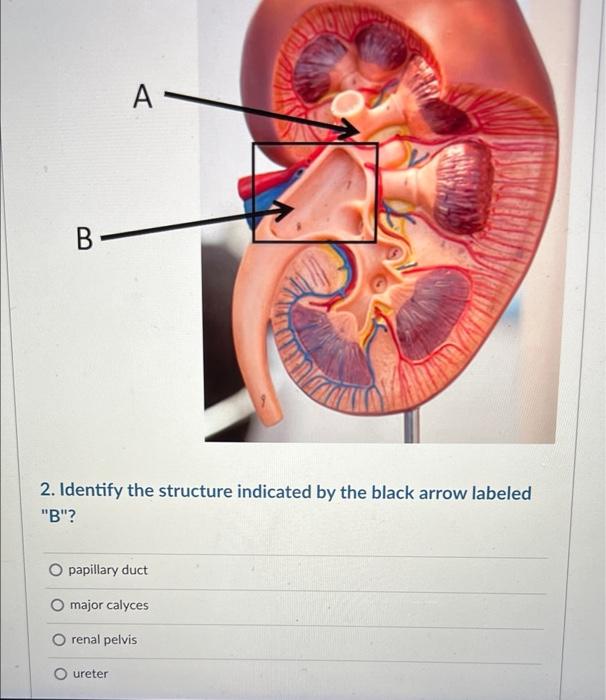
Name the structure marked with an arrow
A 2-year-old child presents with severe acute malnutrition with features of kwashiorkor. Which of the following clinical signs is most indicative of this condition?
A 2 years baby with 6.7 kg, Hb%- 6 g/dl total protein 3 g/dL, low albumin with distended stomach but no proteinuria. What will be the diagnosis?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app