
Nutrition and Health — MCQs

On this page
An 8-month-old infant is being treated with vitamin A supplementation over 2 consecutive days for Vitamin A deficiency. What is the recommended dose to be given each day?
A community health survey reveals that 40% of children under 5 years are stunted, 15% are wasted, and 35% are underweight. Based on these findings, what is the most likely underlying problem in this community?
According to the WHO definition, what is the recommended indicator for assessing the nutritional status of a community?
According to the population strategy for prevention of coronary artery disease, what is the recommended dietary cholesterol intake limit per day?
Under the Weekly Iron and Folic Acid Supplementation (WIFS) scheme, what is the composition of IFA tablets given to children aged 10-19 years?
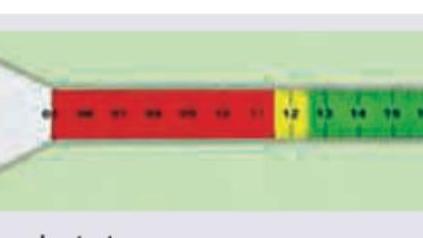
The following instrument is used for the measurement of: (Recent NEET Pattern 2016-17)

The following image shows presence of:

Which of the following can be monitored using this tape?
The Ministry of Health and Family Welfare has launched a programme to meet the challenge of high prevalence of anaemia amongst adolescent boys and girls. Consider the following statements in relation to the key interventions being undertaken : I. It entails supervised weekly administration of 100 mg elemental iron and 500 mu g folic acid. II. These weekly iron-folic acid supplements are administered by using a fixed day approach. III. It entails supervised administration of Albendazole 400 mg every three months for control of helminth infestation. Which of the statements given above is/are correct?
Consider the following statement : "The people should seek to preserve their traditional eating patterns and lifestyles associated with low levels of Coronary Heart Disease (CHD)." Which level of prevention is implied in this statement?
Practice by Chapter
Basic Nutritional Requirements
Practice Questions
Assessment of Nutritional Status
Practice Questions
Protein-Energy Malnutrition
Practice Questions
Micronutrient Deficiencies
Practice Questions
Nutritional Programs in India
Practice Questions
Dietary Guidelines
Practice Questions
Food Safety and Security
Practice Questions
Diet and Non-Communicable Diseases
Practice Questions
Nutrition in Pregnancy and Lactation
Practice Questions
Infant and Young Child Nutrition
Practice Questions
Nutrition in Emergencies
Practice Questions
Food Fortification and Supplementation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app