
Nutrition and Health — MCQs

On this page
Wasting in a child is assessed by which of the following measures?
A community health survey reveals that 40% of children under 5 years are stunted, 15% are wasted, and 35% are underweight. Based on these findings, what is the most likely underlying problem in this community?
According to the WHO definition, what is the recommended indicator for assessing the nutritional status of a community?
Under the Weekly Iron and Folic Acid Supplementation (WIFS) scheme, what is the composition of IFA tablets given to children aged 10-19 years?
Which of the following food adulterant leads to this clinical finding? (Recent NEET Pattern 2016-17)

The following instrument is used for the measurement of: (Recent NEET Pattern 2016-17)

The Food Safety and Standards Act, under which the Food Safety and Standards Authority of India (FSSAI) was established, was enacted in:

The following symbol depicts:

What is the stage of Lathyrism shown below? The patient walks with one stick.

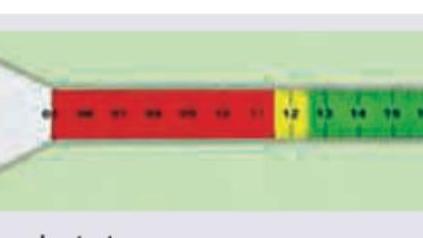
Which of the following can be monitored using this tape?
Practice by Chapter
Basic Nutritional Requirements
Practice Questions
Assessment of Nutritional Status
Practice Questions
Protein-Energy Malnutrition
Practice Questions
Micronutrient Deficiencies
Practice Questions
Nutritional Programs in India
Practice Questions
Dietary Guidelines
Practice Questions
Food Safety and Security
Practice Questions
Diet and Non-Communicable Diseases
Practice Questions
Nutrition in Pregnancy and Lactation
Practice Questions
Infant and Young Child Nutrition
Practice Questions
Nutrition in Emergencies
Practice Questions
Food Fortification and Supplementation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app