
Nutrition and Health — MCQs

On this page
Iodine status in a population is best measured using which of the following?
What is the recommended percentage of fat intake in a prudent diet?
Height in centimeters divided by the cube root of body weight is also known as which index?
Which of the following are suggestions to improve the nutritional value of the Mid-day meal program?
Which food source has the highest biological value?
Which of the following processes prevents lathyrism from Khesari dal?
According to WHO, what is the cut-off for the diagnosis of anemia in non-pregnant females?
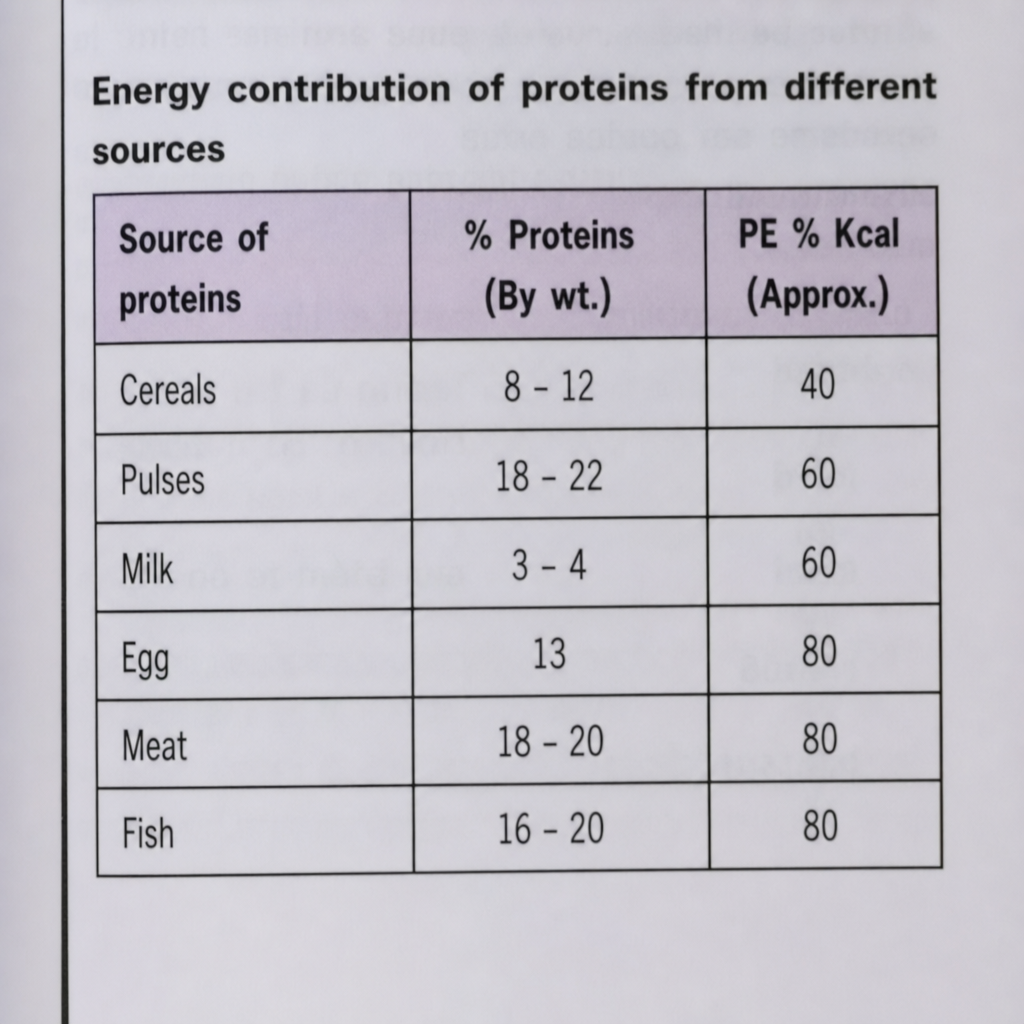
What is the percent of total energy supplied by fish protein (PE % Kcal)?
Which of the following is not present in pulses?
What is the recommended daily iodine intake for pregnant women?
Practice by Chapter
Basic Nutritional Requirements
Practice Questions
Assessment of Nutritional Status
Practice Questions
Protein-Energy Malnutrition
Practice Questions
Micronutrient Deficiencies
Practice Questions
Nutritional Programs in India
Practice Questions
Dietary Guidelines
Practice Questions
Food Safety and Security
Practice Questions
Diet and Non-Communicable Diseases
Practice Questions
Nutrition in Pregnancy and Lactation
Practice Questions
Infant and Young Child Nutrition
Practice Questions
Nutrition in Emergencies
Practice Questions
Food Fortification and Supplementation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app