
Nutrition and Health — MCQs

On this page
Based on epidemiological studies, which of the following has been found to be most protective against carcinoma of the colon?
Which of the following is the richest source of Vitamin C?
What is the Body Mass Index (BMI) of a 46-year-old man who weighs 98kg and is 175cm tall?
Which of the following findings does NOT indicate poor nutrition in children?
Soya bean is rich in which of the following amino acids?
Which of the following statements about the Gomez classification of malnutrition is false?
Dietary Reference Intake recommendations include all of the following except:
What is the most immediate treatment for night blindness?
Which of the following statements is FALSE?
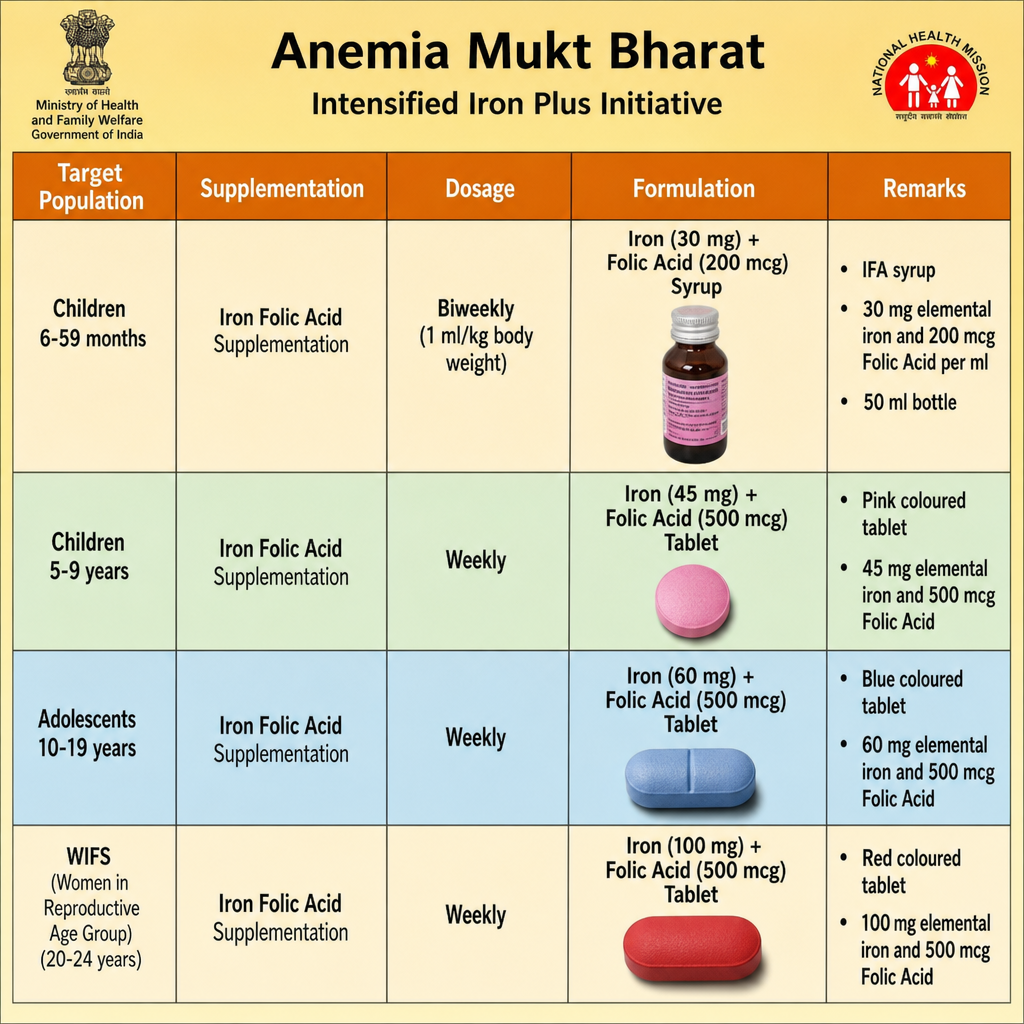
Which of the following statements is true regarding the given program?
Practice by Chapter
Basic Nutritional Requirements
Practice Questions
Assessment of Nutritional Status
Practice Questions
Protein-Energy Malnutrition
Practice Questions
Micronutrient Deficiencies
Practice Questions
Nutritional Programs in India
Practice Questions
Dietary Guidelines
Practice Questions
Food Safety and Security
Practice Questions
Diet and Non-Communicable Diseases
Practice Questions
Nutrition in Pregnancy and Lactation
Practice Questions
Infant and Young Child Nutrition
Practice Questions
Nutrition in Emergencies
Practice Questions
Food Fortification and Supplementation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app