
Infectious Diseases — MCQs

On this page
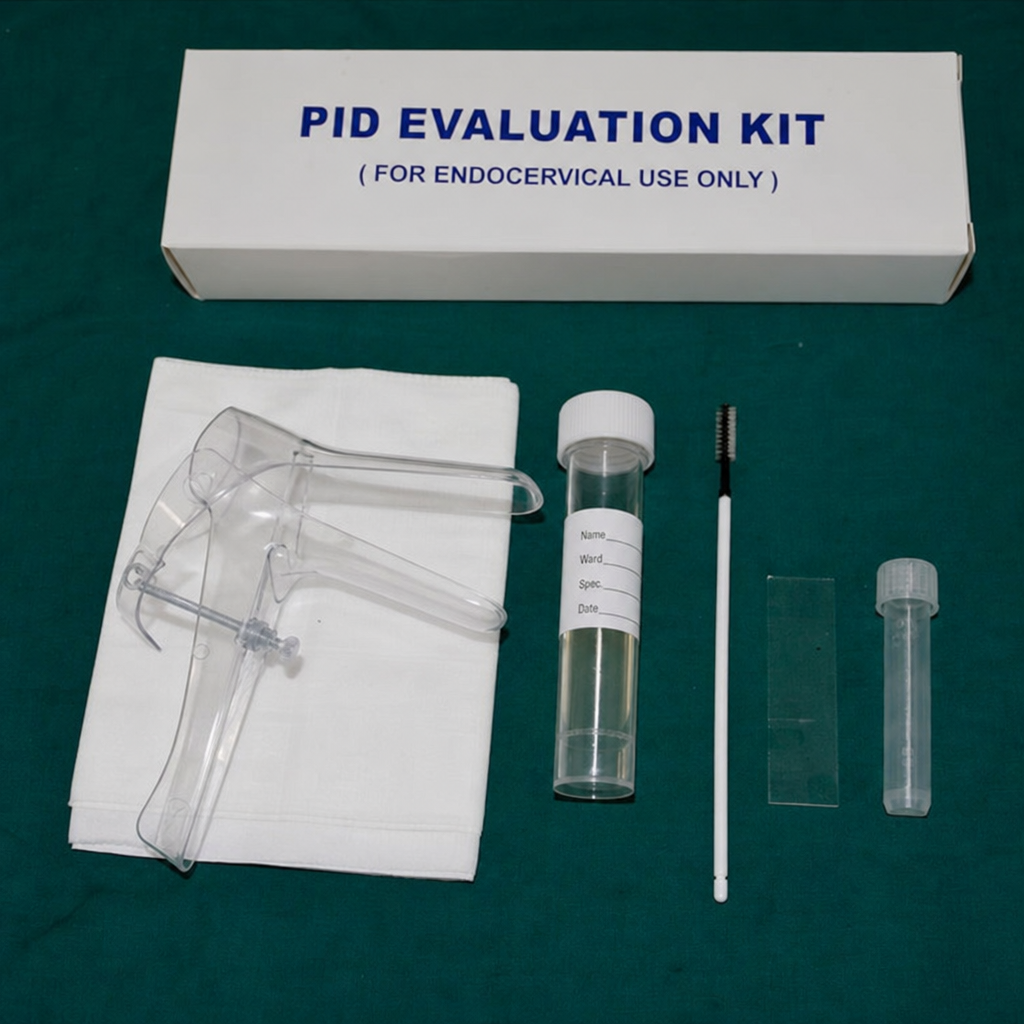
The kit shown in the picture is used for treatment of:

The kit shown here is used for evaluation of which of the following? (AIIMS Nov 2017)
A sexually active adult presents with an acute, painful, unilateral groin swelling. Examination shows enlarged, tender, fluctuant inguinal lymph nodes; a preceding genital ulcer may have already healed. Under the NACO syndromic approach to STI/RTI management, which syndrome does this presentation represent?
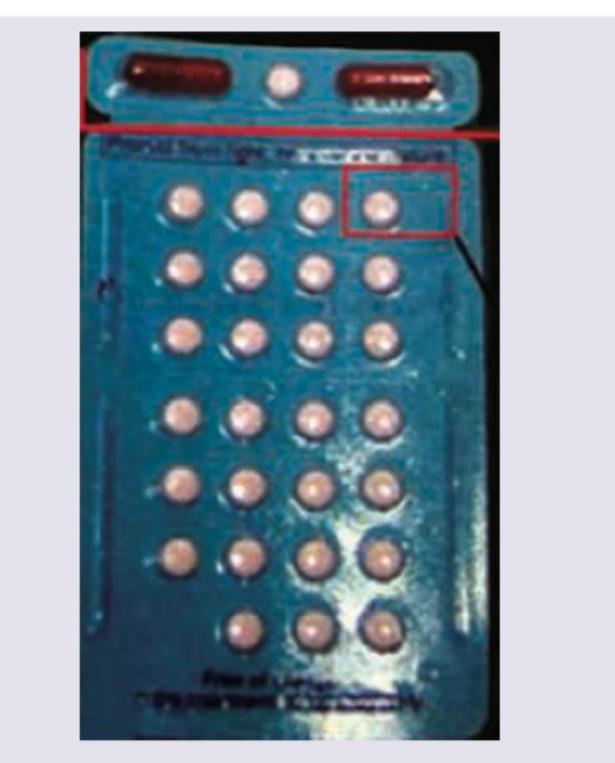
The following leprosy kit is used for management of:
A housefly transmits any infectious agent by which of the following methods, most commonly?
Which of the following mosquito-borne diseases are transmitted chiefly by Aedes mosquito ? 1. Dengue 2. West Nile fever 3. Yellow fever 4. Zika fever Select the correct answer using the code given below :
In which one of the following diseases, the transmission chain is 'Man-Snail-Man' ?
Which of the following statements are correct regarding Chikungunya fever ? 1. It is usually transmitted by Culex mosquito. 2. A safe and effective vaccine is available for commercial use. 3. Incubation period is 4 - 7 days. 4. One of the prominent symptoms is arthropathy. Select the correct answer using the code given below :
A water body was inspected to look for the presence of mosquito eggs. It was observed that there were boat-shaped eggs, laid singly, not in clusters. The eggs also had lateral floats. Which one of the following diseases is most likely to be spread by the mosquito whose eggs were found ?
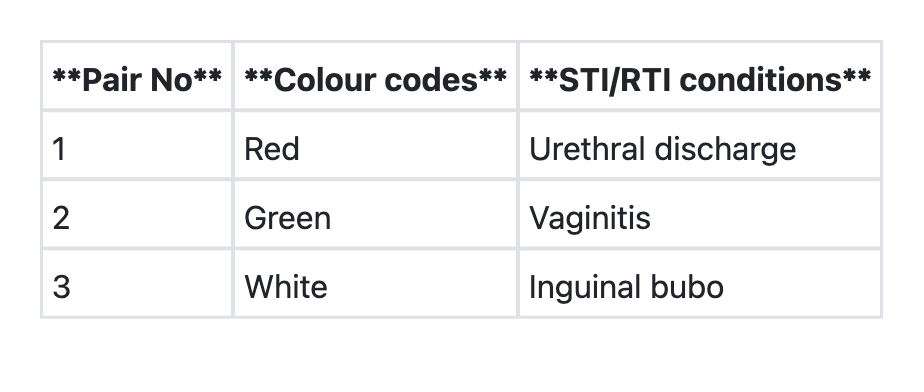
The National AIDS Control Organization provides prepacked colour-coded STI/RTI kits as a free supply to its designated STI/RTI clinics. Consider the following pairs: Pair No Colour codes STI/RTI conditions 1 Red Urethral discharge 2 Green Vaginitis 3 White Inguinal bubo How many of the pairs given above are correctly matched?
Practice by Chapter
Communicable Disease Control Principles
Practice Questions
Vector-Borne Diseases
Practice Questions
Water-Borne Diseases
Practice Questions
Air-Borne Diseases
Practice Questions
Zoonotic Diseases
Practice Questions
Sexually Transmitted Infections
Practice Questions
HIV/AIDS Control Program
Practice Questions
Tuberculosis Control
Practice Questions
Leprosy Elimination
Practice Questions
Emerging and Re-emerging Infections
Practice Questions
Hospital-Acquired Infections
Practice Questions
Integrated Disease Surveillance Project
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app