
Immunization and Vaccine-Preventable Diseases — MCQs

On this page
Consider the following statements regarding Vaccine Vial Monitor (VVM) on the vial of oral polio vaccine : The vaccine is not potent and should be discarded 1. if the colour of the small square within the circle is lighter in colour than that of the circle 2. if the small square within the circle is of the same colour as the circle 3. if the small square within the circle is darker in colour than the colour of the circle Which of the statements given above is/are correct?
Which one of the following is an absolute contraindication for administration of killed vaccine?
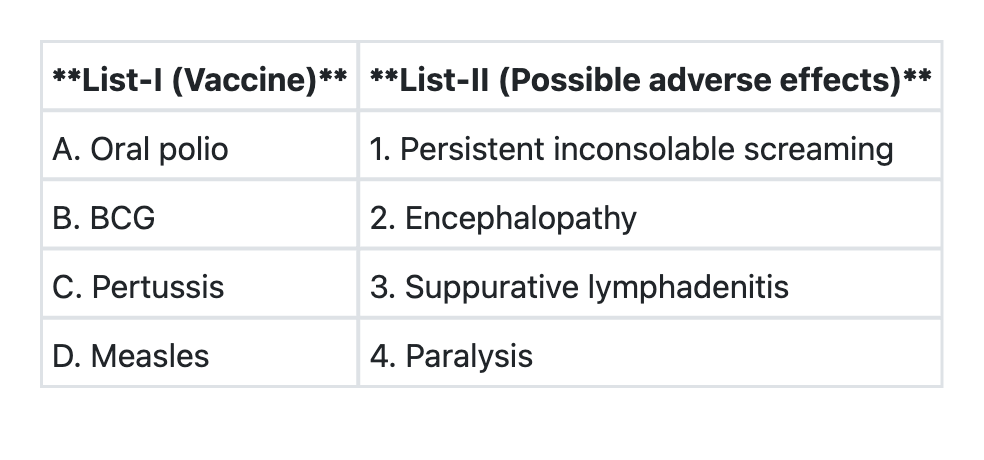
Match List-I with List-II and select the correct answer using the code given below the Lists:
Which of the following vaccines has NOT been introduced in the Universal Immunization Programme in India?
With reference to Vaccine Vial Monitors (VVM) being used on vaccine vials, which of the following statements is/are correct? 1. It gives information about heat exposure over a period of time 2. It directly indicates vaccine potency Select the correct answer using the code given below:
At the end of an immunization session, you found that a reconstituted BCG vaccine vial has around two doses left in it. What should be done in such a situation?
Which is the first step in carrying out an Adverse Event Following Immunization (AEFI)?
A pregnant woman visits a medical officer for an antenatal check up. The woman mentions that she had received two doses of Tetanus Toxoid vaccine four years ago. Which of the following steps should the medical officer take with regard to administration of Tetanus Toxoid vaccine as per the Government of India recommended schedule?
Due to a measles outbreak in a community, a medical officer decided to immunize a child aged seven months with measles vaccine. When should the next measles vaccine be administered?
Which of the following vaccines are given through the intramuscular route? 1. BCG vaccine 2. Hepatitis B vaccine 3. Pentavalent vaccine 4. Inactivated Polio vaccine
Practice by Chapter
Principles of Immunization
Practice Questions
Types of Vaccines
Practice Questions
Universal Immunization Program
Practice Questions
Cold Chain System
Practice Questions
Vaccine Storage and Handling
Practice Questions
Adverse Events Following Immunization
Practice Questions
National Immunization Schedule
Practice Questions
Polio Eradication
Practice Questions
Measles Elimination
Practice Questions
Tetanus Control
Practice Questions
New and Underutilized Vaccines
Practice Questions
Vaccination Coverage Assessment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app