
Immunization and Vaccine-Preventable Diseases — MCQs

On this page
What is true about polio?
Which of the following statements is NOT true about the Inactivated Polio Vaccine (IPV)?
Which of the following vaccines is the most effective?
Which of the following vaccines, if contaminated, can cause Toxic Shock Syndrome (TSS)?
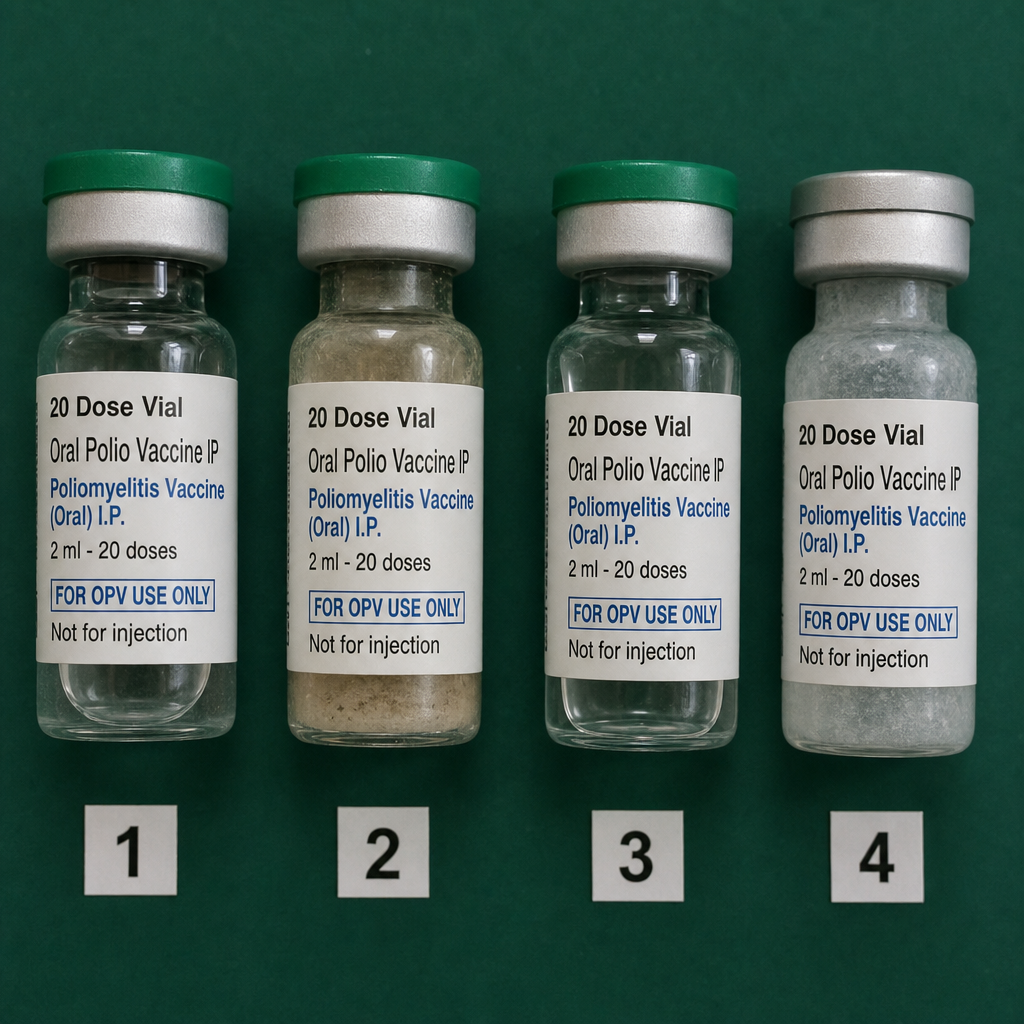
Which of the following Oral Polio Vaccine (OPV) vials are usable?
What is the post-exposure prophylaxis schedule for rabies vaccine in a previously immunized person?
How many vaccine vials can a carrier transport daily?
A 3-year-old, completely unimmunized child presents to a primary health center immunization clinic for the first time. Which vaccines should be administered?
Which of the following vaccines does not provide herd immunity?
What is the principle behind supplementary immunisation services for measles immunisation?
Practice by Chapter
Principles of Immunization
Practice Questions
Types of Vaccines
Practice Questions
Universal Immunization Program
Practice Questions
Cold Chain System
Practice Questions
Vaccine Storage and Handling
Practice Questions
Adverse Events Following Immunization
Practice Questions
National Immunization Schedule
Practice Questions
Polio Eradication
Practice Questions
Measles Elimination
Practice Questions
Tetanus Control
Practice Questions
New and Underutilized Vaccines
Practice Questions
Vaccination Coverage Assessment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app