
Immunization and Vaccine-Preventable Diseases — MCQs

On this page
Which vaccine is contraindicated in pregnancy?
A PLHIV came with multiple dog bites with a punctured wound. Choose the correct management:
Which of the following is the schedule of the OPV vaccine?
A patient comes with a history of category 3 dog bites. He received prophylaxis for a monkey bite 6 months back. What is the next step in management?
Which of the following vials, as shown in the image, can be used for administering vaccines?
The accompanying portrait is an unverified artistic illustration for a museum display about the 1796 experiment in which material from a cowpox lesion was used to protect against smallpox. Which historical figure should the display identify as the investigator who performed this experiment?
All are correct regarding the live attenuated intranasal influenza vaccine (LAIV) except:
A child has developed this complication after vaccination. Which is the vaccine responsible?

All are correct about the vaccine shown except (per CDC/ACIP guidelines):
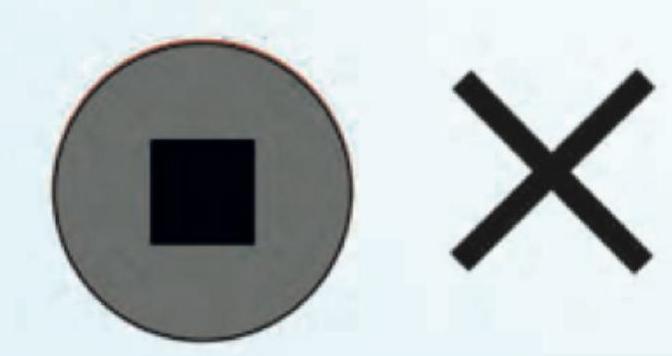
Which is correct about the Vaccine Vial monitor shown in the image? (Recent NEET Pattern 2016-17)
Practice by Chapter
Principles of Immunization
Practice Questions
Types of Vaccines
Practice Questions
Universal Immunization Program
Practice Questions
Cold Chain System
Practice Questions
Vaccine Storage and Handling
Practice Questions
Adverse Events Following Immunization
Practice Questions
National Immunization Schedule
Practice Questions
Polio Eradication
Practice Questions
Measles Elimination
Practice Questions
Tetanus Control
Practice Questions
New and Underutilized Vaccines
Practice Questions
Vaccination Coverage Assessment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app