
Health Policy and Management — MCQs

On this page
The degree to which a specific health care intervention achieves its objectives, when applied in a given population, is termed as its
The National Health Policy 2002 target to be achieved by the year 2010 is :
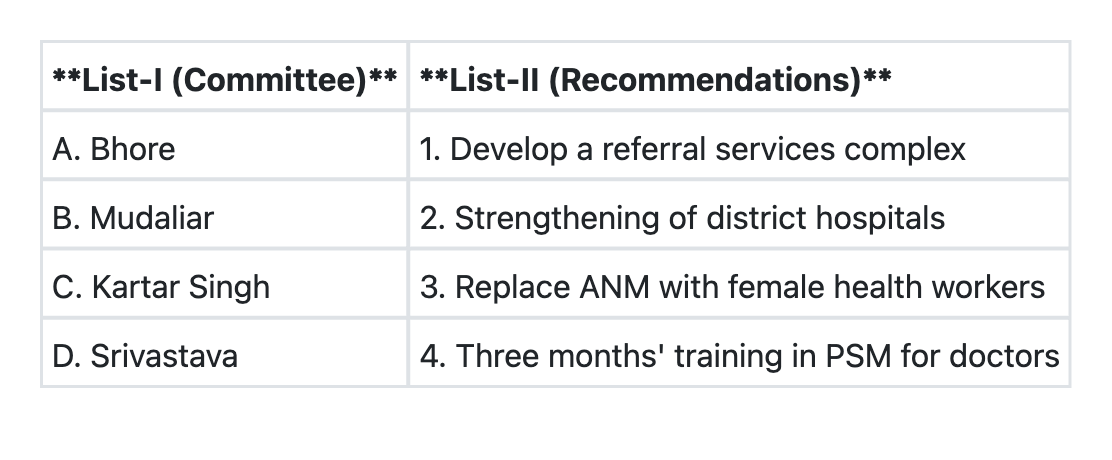
Match List-I with List-II and select the correct answer using the code given below the Lists:
Suraksha Clinics are conducted under the aegis of which National Health Programme?
Which National Programme came into existence during 11th Five Year Plan?
The following are objectives of Indian Public Health Standards for Primary Health Centres except:
Which one of the following is a quantitative method of health management?
The following are the principles of Primary Health Care except:
Which of the following is NOT a quantitative method in the management of health services?
With reference to the Revised National Tuberculosis Control Programme, consider the following statements: 1. Active case finding is pursued under this Programme. 2. Microscopy centres are established in the districts for every one lakh population and in hilly and tribal areas for every 50,000 population. Which of these statements is/are correct?
Practice by Chapter
Health Systems and Models
Practice Questions
Health Planning Process
Practice Questions
Health Program Implementation
Practice Questions
Health Economics
Practice Questions
Health Financing Methods
Practice Questions
Healthcare Resource Allocation
Practice Questions
Quality Assessment in Healthcare
Practice Questions
Health Insurance Models
Practice Questions
Public-Private Partnerships
Practice Questions
Universal Health Coverage
Practice Questions
Healthcare Leadership
Practice Questions
Health Policy Evaluation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app