
Health Policy and Management — MCQs

On this page
All of the following are dashboard indicators used for monitoring of India Newborn Action Plan (INAP). Which one of them is an impact level indicator ?
The cost of implementation of 'Ayushman Bharat Pradhan Mantri Jan Arogya Yojana' is borne by :
Consider the following statements with regard to selection of Accredited Social Health Activist (ASHA) under NRHM : 1. ASHA must be a woman preferably of age 18 to 25 years. 2. ASHA should be married. 3. ASHA must be a resident of the village. 4. ASHA may be a married, widowed or divorced woman. Which of the statements given above are correct with regard to process of selection of ASHA?
Consider the following statements regarding the Central Drugs Standard Control Organization (CDSCO) in India : 1. The CDSCO is headed by the Drugs Controller General (India) at the Centre. 2. The CDSCO is a part of the Directorate of Director General of Health Services. 3. The CDSCO is under the Ministry of Chemicals and Fertilizers, Government of India. 4. The CDSCO has a network of several port offices for monitoring the import and export of drugs. Which of the statements given above are correct?
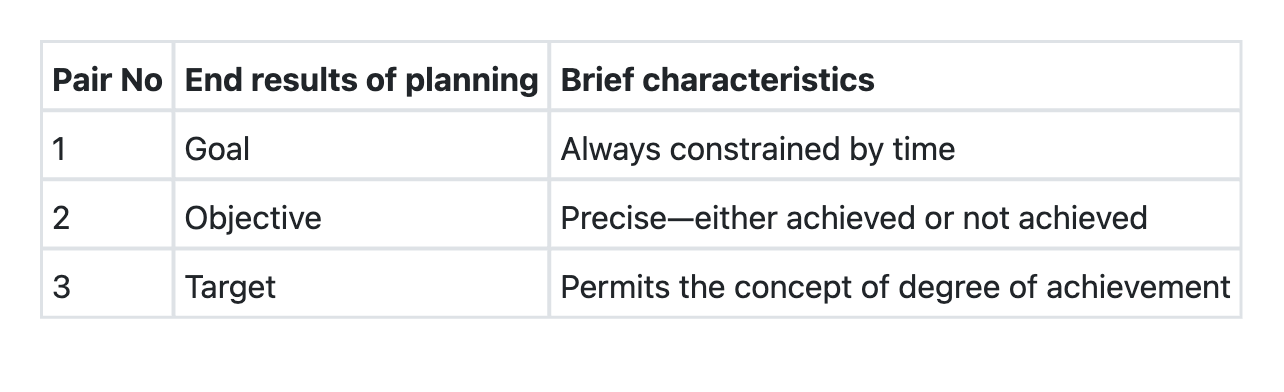
In the following table, the end results of planning are qualified by brief characteristics. How many of the pairs given above are correctly matched?
The table given below shows three broad components under which the objectives of the National Health Policy, 2017 can be grouped, along with examples of goals/objectives under each component. How many of the pairs shown in the table are correctly matched? Select the correct answer using the code given below.

Consider the following statements with reference to the National Framework for Malaria Elimination in India, 2016–2030. Which of the following statements is correct? 1. The goal is to eliminate indigenous cases throughout the country by 2030. 2. By 2022, transmission of malaria is to be interrupted and indigenous cases brought to zero in all 26 States/UTs that were under Categories 1 and 2 in 2014. 3. By 2026, incidence of malaria is to be reduced to less than 1 case per 1000 population in all States and UTs, and their districts. 4. By 2030, indigenous transmission of malaria is to be interrupted in all States and UTs of India.
Which of the following statements is true about 'End TB Strategy'?
Which one of the following is not a utilization rate ?
Which of the following countries was the first to institute compulsory sickness insurance?
Practice by Chapter
Health Systems and Models
Practice Questions
Health Planning Process
Practice Questions
Health Program Implementation
Practice Questions
Health Economics
Practice Questions
Health Financing Methods
Practice Questions
Healthcare Resource Allocation
Practice Questions
Quality Assessment in Healthcare
Practice Questions
Health Insurance Models
Practice Questions
Public-Private Partnerships
Practice Questions
Universal Health Coverage
Practice Questions
Healthcare Leadership
Practice Questions
Health Policy Evaluation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app