
Health Education and Communication — MCQs

On this page
Which among the following are characteristics of health education, rather than propaganda? 1. Knowledge actively acquired, rather than instilled 2. Appeals to emotion, rather than reason 3. Behaviour centred, rather than information centred 4. Arouses and stimulates primitive desires, rather than disciplines them Select the correct answer using the code given below.
The attitude is a domain of:
Direct mailing as a means of communication, is an example of:
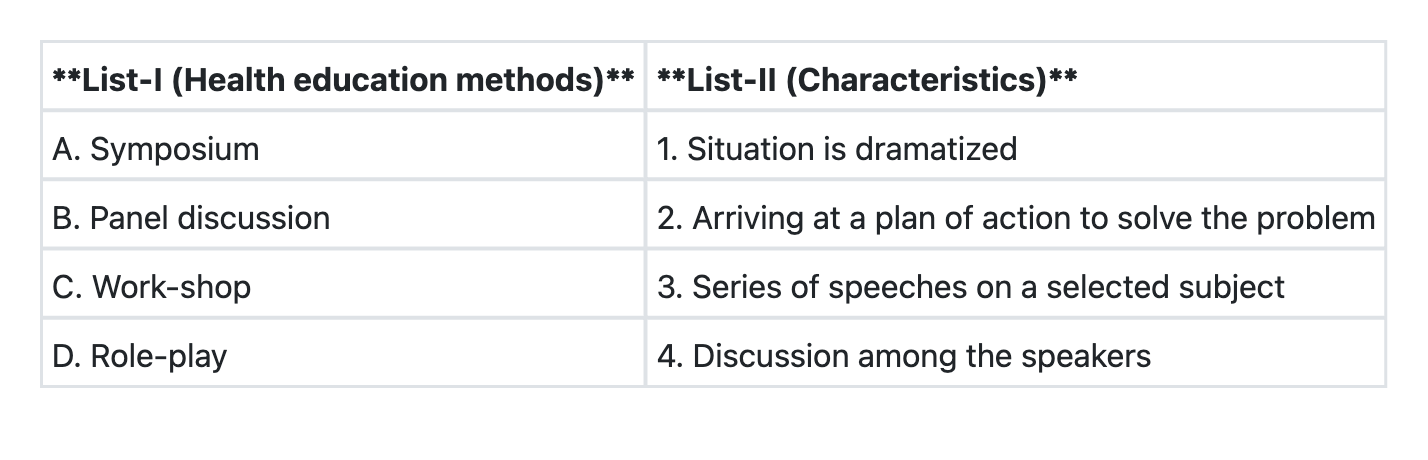
Match List-I with List-II and select the correct answer using the code given below the Lists:
In healthcare settings, a series of meetings where individuals work within small groups to arrive at a plan of action for addressing health problems or implementing interventions is called
Which of the following is NOT a mass approach in health communication?
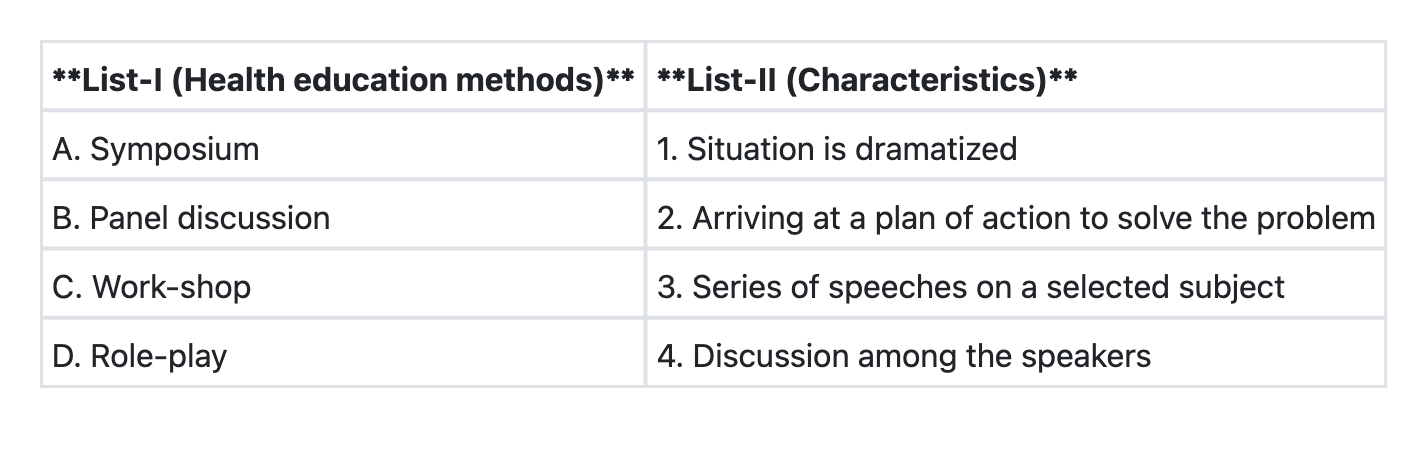
Match List-I with List-II and select the correct answer using the code given below the Lists:
Consider the following statements: Symposium is a method of health education characterised by 1. a series of speeches on a selected topic 2. presentation of different aspects of a topic by 3 or 4 experts. 3. a discussion among the symposium members 4. the chairperson making a comprehensive summary at the end of the session Which of these statements are correct?
All of the following are mass approaches towards education of general public EXCEPT:
In a basic Health Education model, the first step is Awareness, and the second step is Motivation. What is the third step?
Practice by Chapter
Principles of Health Education
Practice Questions
Communication Theories
Practice Questions
Methods of Health Education
Practice Questions
Planning Health Education Programs
Practice Questions
Audio-Visual Aids
Practice Questions
Mass Media in Health Communication
Practice Questions
Information, Education, and Communication (IEC)
Practice Questions
Behavior Change Communication (BCC)
Practice Questions
Social Media in Health Education
Practice Questions
Evaluation of Health Education Programs
Practice Questions
Health Literacy
Practice Questions
Risk Communication
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app