
Health Economics — MCQs

On this page
In a programme, analysis of results in comparison to cost is known as
What is the most cost-effective screening for identifying carcinoma cervix in a population?
Which one of the following is a quantitative method of health management?
Which one among the following was used for measuring economic status of households, in the National Family Health Survey-III (NFHS-III) ?
The life expectancy at birth for a country A is 64 years. The minimum and maximum values of life expectancy are 20 years and 86 years respectively. As part of Human Development Index (HDI), what is the Life Expectancy Index for the country A ?
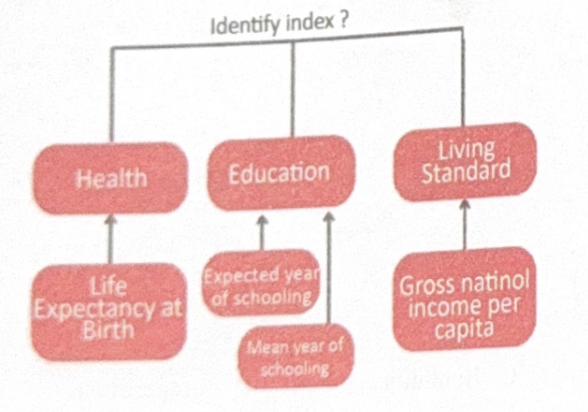
Identify the index?
Which intervention has shown the highest return on investment in national STI control programs?
Which of the following evaluation methods primarily involves monetary terms?
In ESI, employee contributes what percentage of wages?
Which of the following best describes economic blindness?
Practice by Chapter
Basic Concepts in Health Economics
Practice Questions
Health Financing Mechanisms
Practice Questions
Cost-Benefit Analysis
Practice Questions
Cost-Effectiveness Analysis
Practice Questions
Health Insurance Systems
Practice Questions
National Health Accounts
Practice Questions
Healthcare Market Analysis
Practice Questions
Economic Evaluation of Health Programs
Practice Questions
Resource Allocation in Healthcare
Practice Questions
Direct and Indirect Health Costs
Practice Questions
Health Budget Planning
Practice Questions
Economic Burden of Disease
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app