
Economic Evaluation of Health Programs — MCQs

Based on healthcare utility values and life expectancy, which of the following measures can be calculated? Consider a scenario where the average life expectancy for a woman in Japan is 87 years, and there is an increase in life expectancy due to healthcare advancements.
In implementation of a health programme, best thing to do is -
The disability adjusted life years (DALYs) lost due to neuropsychiatric disorders are highest in -
Disability-adjusted life years (DALYs) measure the burden of disease by accounting for both:
Which of the following statements is TRUE regarding Disability-Adjusted Life Year (DALY)?
Which of the following is not considered a participatory approach to health education?
Which of the following is NOT considered an element of primary healthcare?
In a programme, analysis of results in comparison to cost is known as
The most comprehensive indicator of cost-effectiveness analysis is
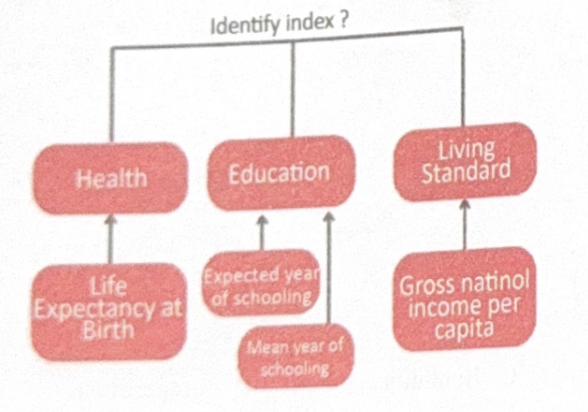
Identify the index?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app