
Environmental Health — MCQs

On this page
The following instrument is used for:
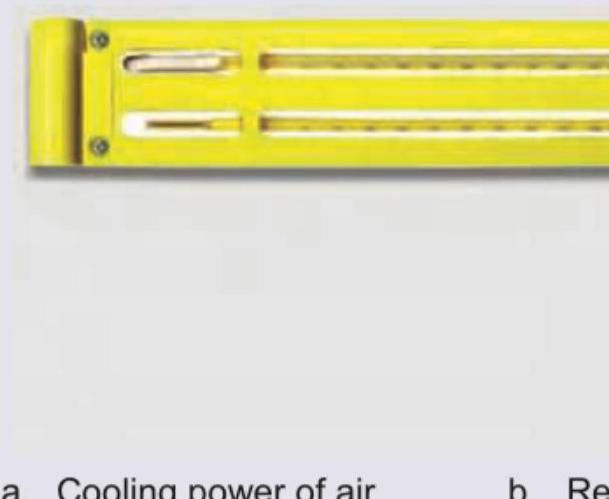
Identify the instrument shown below.

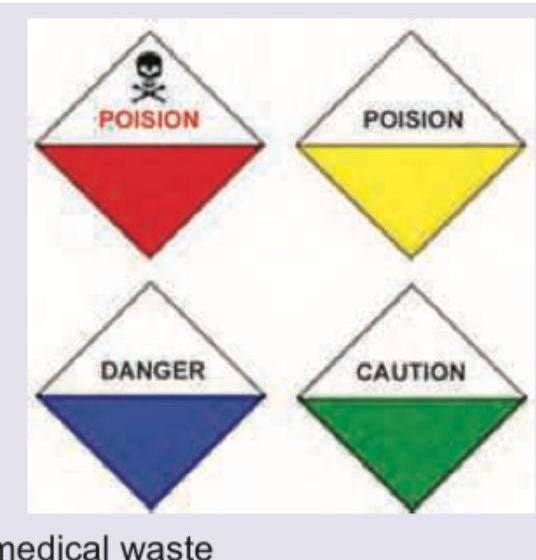
Identify symbol given in the image below:

The image given below is symbolic of:
The symbols shown in the image represent which types of biomedical waste?

The medical officer at a PHC in a fluorosis-endemic district has seen a large number of cases with the following presentation in the last 6 months. Which illness should he be concerned about? (Recent NEET Pattern 2016-17)

The biomedical waste category for the used bone marrow needle shown in the image is:

What are the reasons for choosing coliform organisms as indicators of faecal pollution of water rather than the waterborne pathogens directly? I. They are present in great abundance in the human intestine and excreted in great numbers in faeces. II. They have lower resistance to forces of natural purification. III. They survive lesser than the pathogens. IV. They are easily detected by culture methods. Select the correct answer using the code given below :
Under the Biomedical Waste Management Rules 2016, human anatomical waste is to be carried in which colour plastic bags?
How much illumination is recommended by the Illuminating Engineering Society for general office work?
Practice by Chapter
Water Quality and Health
Practice Questions
Air Pollution and Health Effects
Practice Questions
Solid Waste Management
Practice Questions
Hazardous Waste Management
Practice Questions
Housing and Health
Practice Questions
Noise Pollution
Practice Questions
Radiation Health Effects
Practice Questions
Climate Change and Health
Practice Questions
Environmental Impact Assessment
Practice Questions
Disaster Management and Preparedness
Practice Questions
Vector Control
Practice Questions
Environmental Legislation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app