
Vitamin A and Vision — MCQs

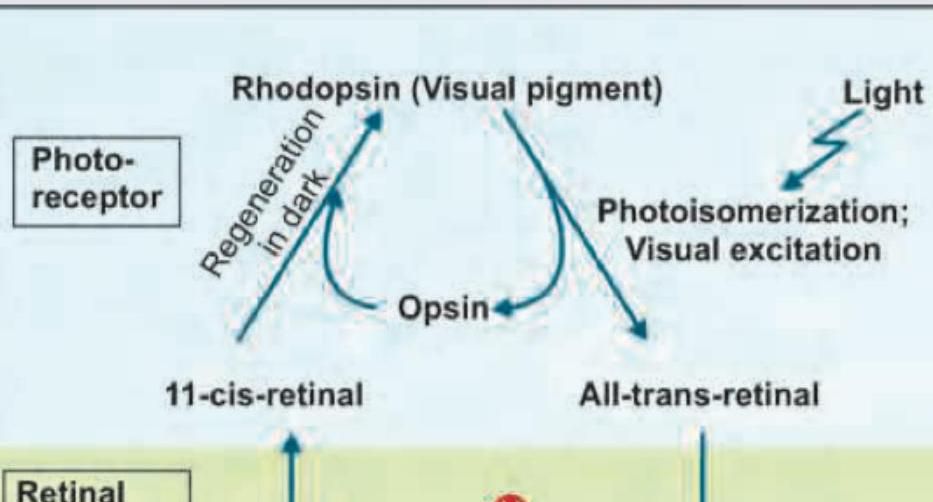
During the dark phase of visual cycle, which form of vitamin A combines with opsin to make Rhodopsin:
Thiamine deficiency is best diagnosed by?
At what age does a child typically know their full name?
Pseudo tumor cerebri is caused by?
A child of 8 kg has Bitot's spots in both eyes. Which of the following is the most appropriate schedule to prescribe vitamin A to this child?
A patient complained of gradual diminution of vision. On examination, the patient had dry eyes and a rough corneal surface. What deficiency is most likely causing these manifestations?
Match the following: A) Caplan syndrome- 1) Found first in coal worker B) Asbestosis- 2) Upper lobe predominance C) Mesothelioma- 3) Involves lower lobe D) Sarcoidosis- 4) Pleural effusion is seen
Name the enzyme involved in this cycle:
All of the following are water-soluble antioxidants except?
A patient presents with recurrent oral lesions and eye redness as shown in the images below. The patient also complains of chronic diarrhea and abdominal discomfort. Which test is recommended for this patient?

Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app