
Vitamins and Coenzymes — MCQs

On this page
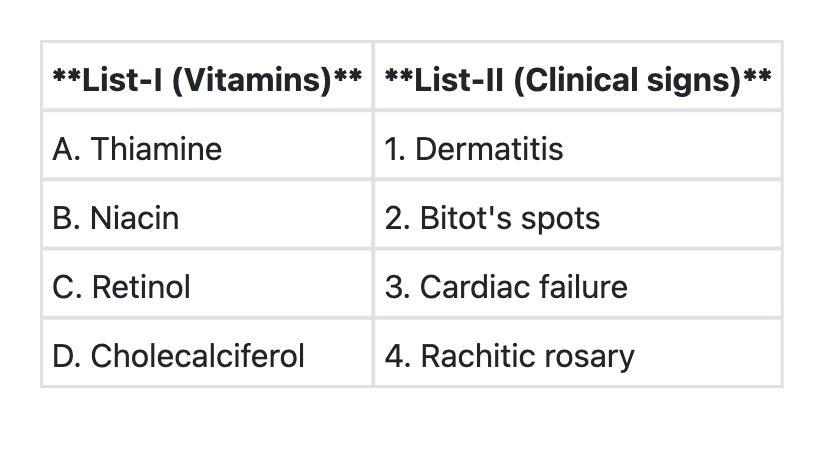
Match List-I with List-II and select the correct answer using the code given below the Lists:
Which one of the following vitamins given as a supplement during the peri-conceptional period to a woman can help prevent the neural tube defects in the baby ?
Consider the following statements: 1. Diets high in vitamin C have been claimed to lower the incidence of certain cancers, particularly oesophageal and gastric cancers. 2. Vitamin C can prevent the conversion of nitrites and secondary amines to carcinogenic nitrosamines. Which of the statements given above is/are correct?
Consider the following statements regarding folic acid: 1. It is needed for normal development of blood cells in the marrow 2. It has a role in synthesis of nucleic acids 3. It is resistant to boiling Which of the above statements is/are correct?
Major source of vitamin K1 is:
Xanthurenic aciduria is seen in which vitamin deficiency?
Methyl-tetrahydrofolate (5-methyl-THF) gets accumulated in deficiency of which of the following?
Most potent lipid phase antioxidant:
Which enzyme level is tested in thiamine deficiency?
Wernicke's encephalopathy is due to deficiency of:
Practice by Chapter
Fat-Soluble Vitamins: A, D, E, K
Practice Questions
Vitamin A and Vision
Practice Questions
Vitamin D and Calcium Metabolism
Practice Questions
Vitamin E and Antioxidant Functions
Practice Questions
Vitamin K and Blood Coagulation
Practice Questions
Water-Soluble Vitamins: B Complex and C
Practice Questions
Thiamine (B1) and Pyruvate Dehydrogenase
Practice Questions
Riboflavin (B2) and Flavin Coenzymes
Practice Questions
Niacin and NAD/NADP
Practice Questions
Vitamin B6 and Transamination
Practice Questions
Folate and Vitamin B12 in One-Carbon Metabolism
Practice Questions
Vitamin C and Collagen Synthesis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app