
Vitamins and Coenzymes — MCQs

On this page
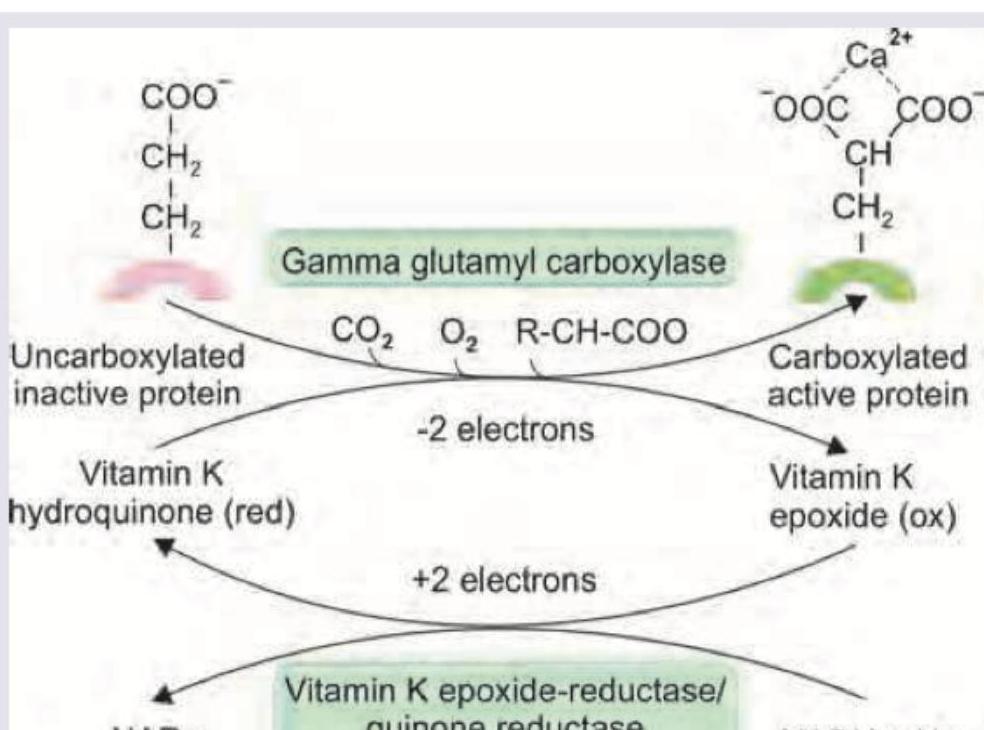
What is correct about the vitamin shown below?
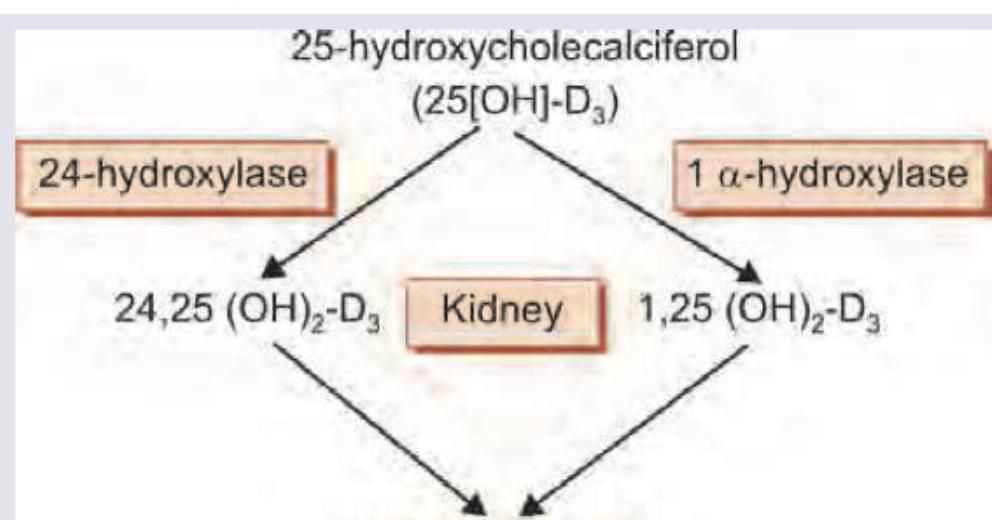
The following reaction occurs in which part of kidney?
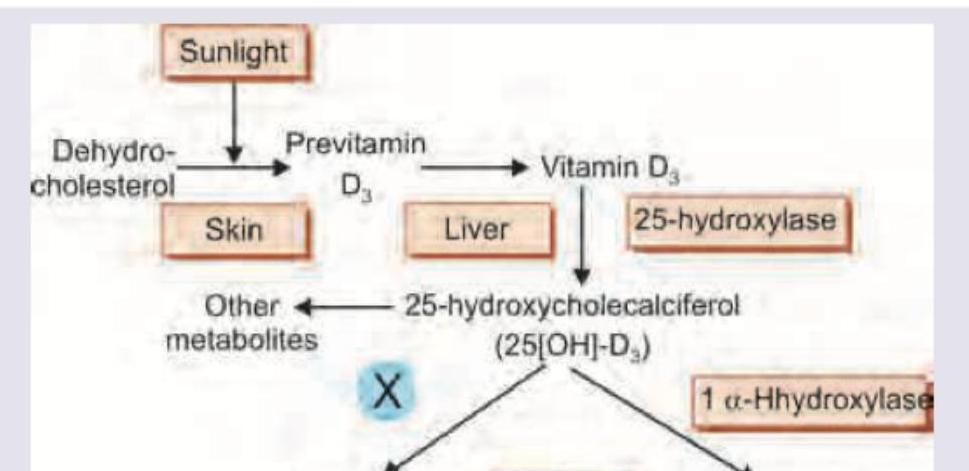
Which enzyme is marked X in the vitamin D metabolic pathway shown below?
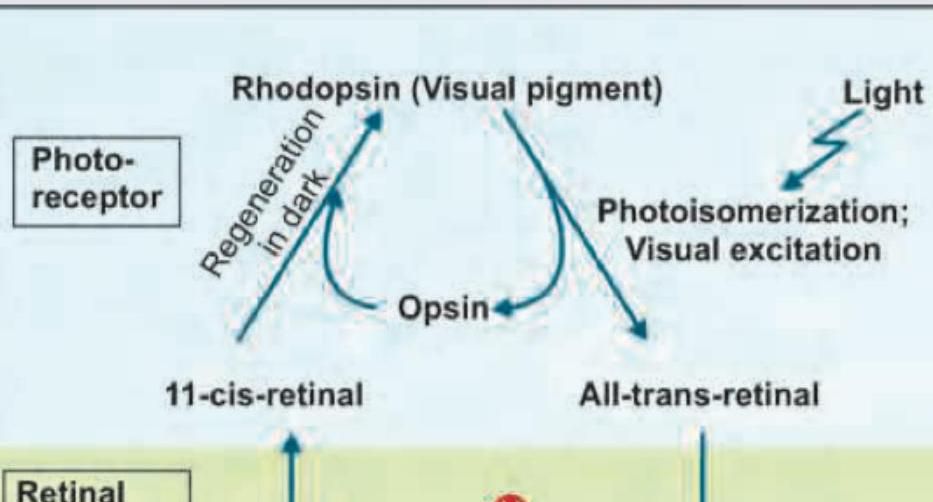
Which enzyme catalyzes the conversion of all-trans-retinyl ester to 11-cis-retinol in the retinal pigment epithelium?
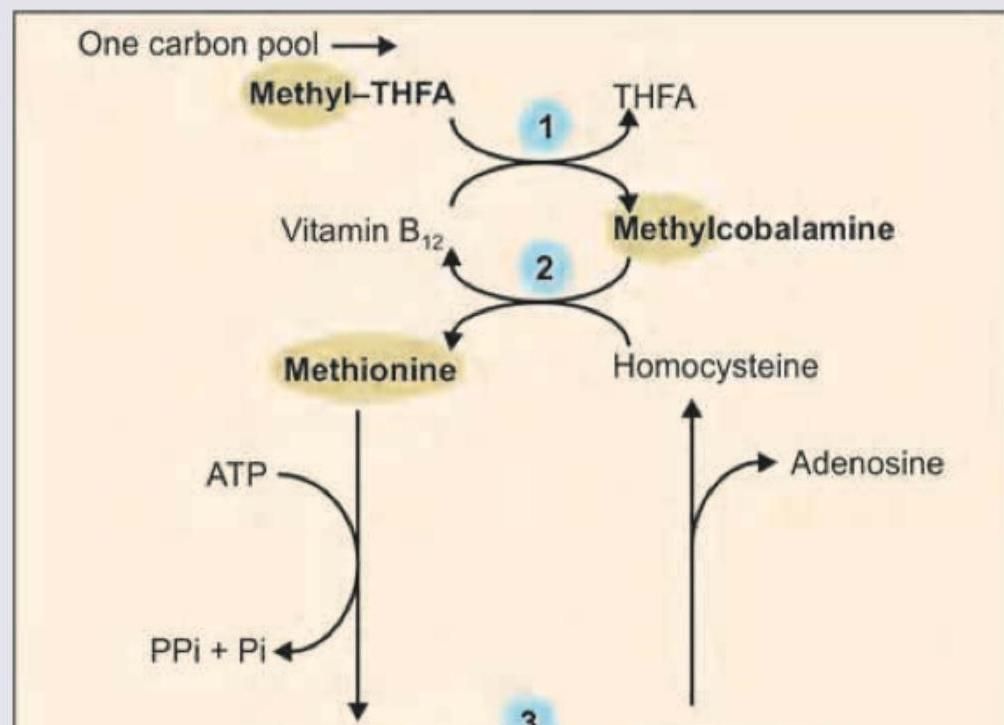
Which of the following reactions is responsible for folate trap?
The following lesion is seen in all of the following conditions except: (Recent NEET Pattern 2016-17)

The bony deformity of 'pigeon chest' in children occurs due to deficiency of:
A 36 year old man presents with decreased appetite, mouth soreness, diarrhoea and irritability. On examination he has a bright red tongue with a pigmented scaly rash around the neck. Which one of the following food items in his diet has a bearing on his disease?
In hyperemesis gravidarum, Wernicke's encephalopathy is seen due to the deficiency of
Consider the following statements : 1. The deficiency of thiamine leads to the accumulation of pyruvic and lactic acids in the body. 2. Riboflavin deficiency impairs the optimal utilization of pyridoxine. Which of the statements given above is/are correct ?
Practice by Chapter
Fat-Soluble Vitamins: A, D, E, K
Practice Questions
Vitamin A and Vision
Practice Questions
Vitamin D and Calcium Metabolism
Practice Questions
Vitamin E and Antioxidant Functions
Practice Questions
Vitamin K and Blood Coagulation
Practice Questions
Water-Soluble Vitamins: B Complex and C
Practice Questions
Thiamine (B1) and Pyruvate Dehydrogenase
Practice Questions
Riboflavin (B2) and Flavin Coenzymes
Practice Questions
Niacin and NAD/NADP
Practice Questions
Vitamin B6 and Transamination
Practice Questions
Folate and Vitamin B12 in One-Carbon Metabolism
Practice Questions
Vitamin C and Collagen Synthesis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app