
Vitamins and Coenzymes — MCQs

On this page
A deficiency of vitamin D can lead to all of the following conditions, except:
Alcoholics may develop fatal lactic acidosis due to inhibition of which of the following enzymes?
A 12-week anomaly scan of a 29-year-old lady revealed fetal malformation. Further investigation revealed she had taken vitamin supplements. Which of the following vitamins is most likely responsible for the fetal defects?
A 4-year-old boy whose diet consists mostly of cheese puffs and cola presents with nyctalopia, xerosis, and headache. Which of the following vitamin or trace element replacement therapies is most appropriate to treat this condition?
Ultrasound examination of a developing fetus demonstrates a fluid-filled sac at the base of the fetus' spine that connects to the spinal canal and apparently contains part of the spinal cord. A dietary deficiency of which of the following is most strongly associated with this type of lesion?
Hypervitaminosis of which of the following vitamins will cause bony abnormalities?
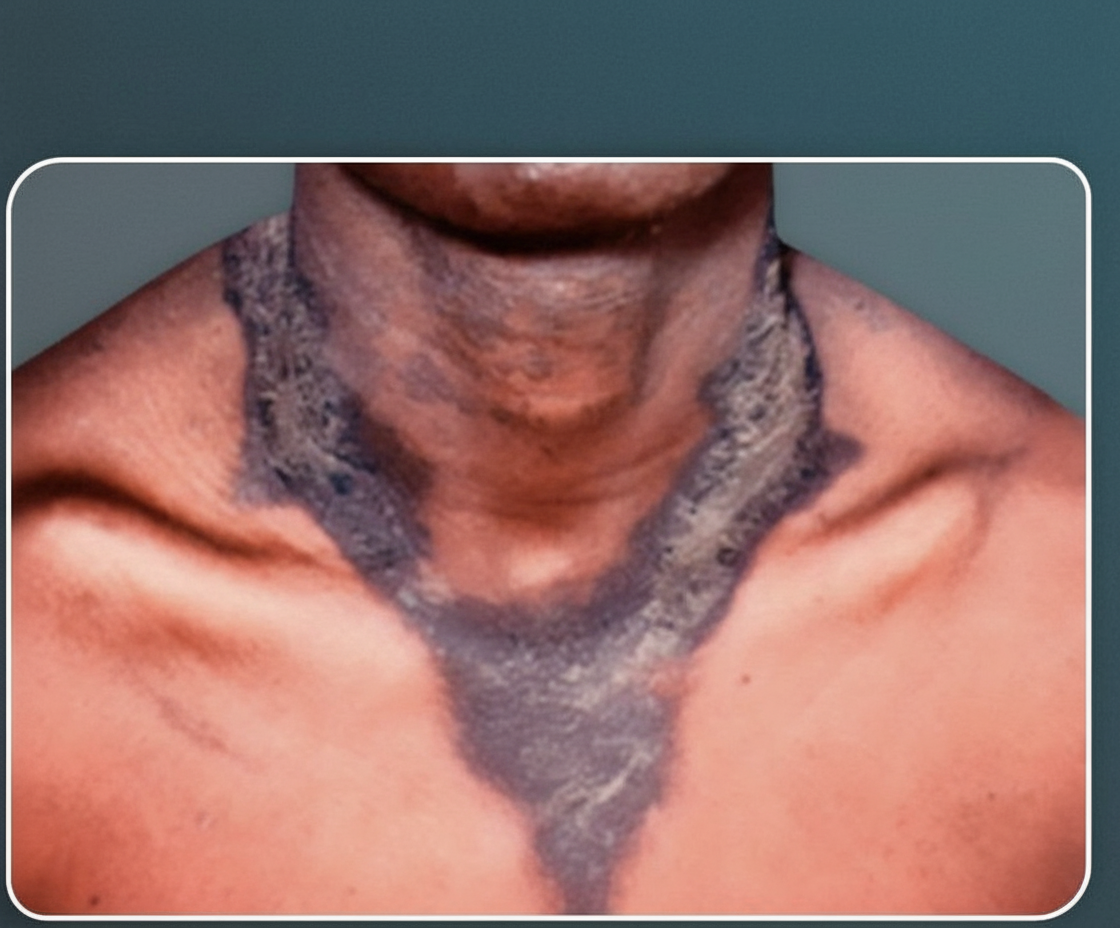
Deficiency of which one of the following dietary components is most likely to have caused this rash?
Which vitamin supplement is used to treat hangovers following alcohol consumption?
Which of the following is the donor of ADP-ribose for ADP-ribosylation reactions?
All of the following are antioxidants except?
Practice by Chapter
Fat-Soluble Vitamins: A, D, E, K
Practice Questions
Vitamin A and Vision
Practice Questions
Vitamin D and Calcium Metabolism
Practice Questions
Vitamin E and Antioxidant Functions
Practice Questions
Vitamin K and Blood Coagulation
Practice Questions
Water-Soluble Vitamins: B Complex and C
Practice Questions
Thiamine (B1) and Pyruvate Dehydrogenase
Practice Questions
Riboflavin (B2) and Flavin Coenzymes
Practice Questions
Niacin and NAD/NADP
Practice Questions
Vitamin B6 and Transamination
Practice Questions
Folate and Vitamin B12 in One-Carbon Metabolism
Practice Questions
Vitamin C and Collagen Synthesis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app