
Vitamins and Coenzymes — MCQs

On this page
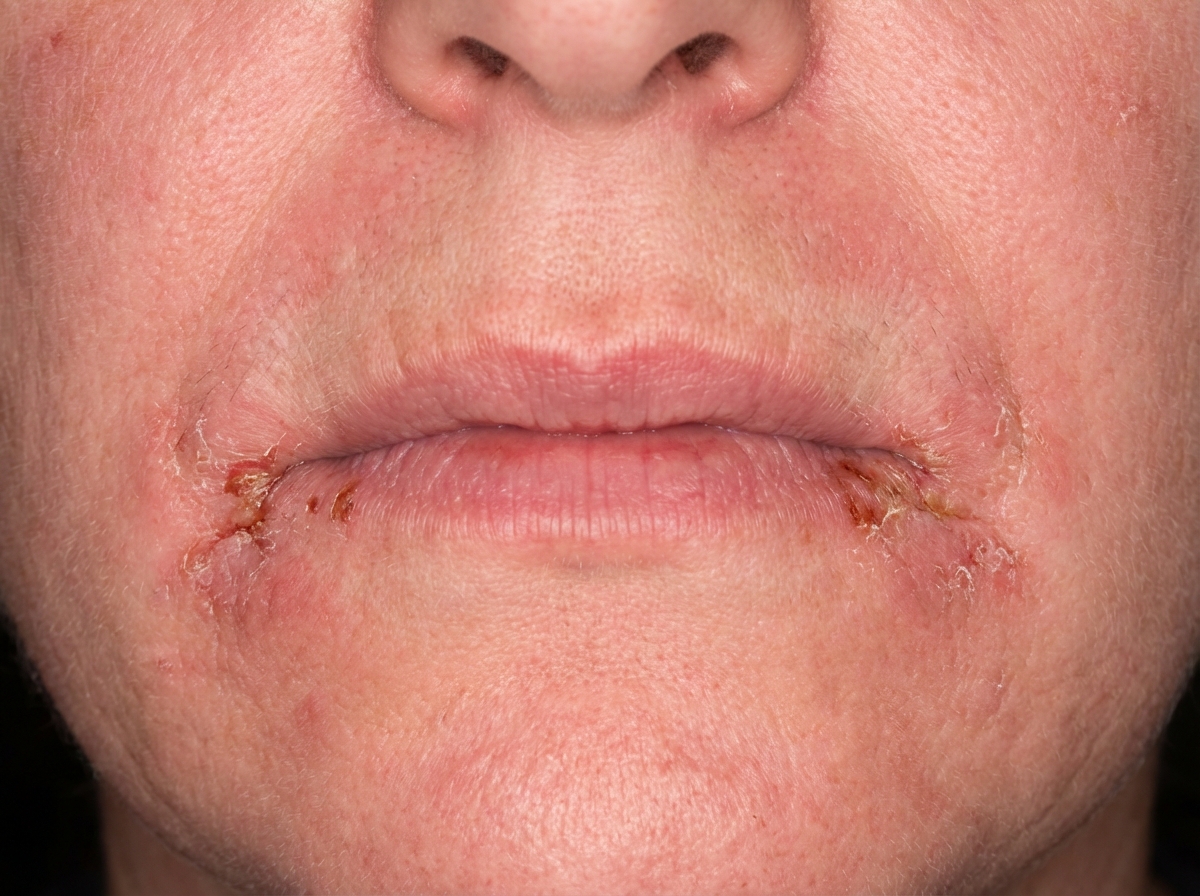
Which vitamin deficiency is most classically associated with this condition?
Which of the following is NOT a form of Vitamin K?
Which nutritional deficiency is associated with hereditary ataxia?
Which vitamin deficiency disorder is associated with a diet primarily consisting of cereals?
Which of the following vitamins does not play any role in the process of tooth development?
Niacin deficiency causes all of the following except?
Which one of the following is not a cause of vitamin B12 deficiency?
Pyridoxal phosphate is a key cofactor in metabolism. Which of the following reactions requires this cofactor?
Vitamin-B12 deficiency is not seen in which of the following conditions?
Which vitamin is essential for the metabolism of sulfur-containing amino acids?
Practice by Chapter
Fat-Soluble Vitamins: A, D, E, K
Practice Questions
Vitamin A and Vision
Practice Questions
Vitamin D and Calcium Metabolism
Practice Questions
Vitamin E and Antioxidant Functions
Practice Questions
Vitamin K and Blood Coagulation
Practice Questions
Water-Soluble Vitamins: B Complex and C
Practice Questions
Thiamine (B1) and Pyruvate Dehydrogenase
Practice Questions
Riboflavin (B2) and Flavin Coenzymes
Practice Questions
Niacin and NAD/NADP
Practice Questions
Vitamin B6 and Transamination
Practice Questions
Folate and Vitamin B12 in One-Carbon Metabolism
Practice Questions
Vitamin C and Collagen Synthesis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app