
Lipid Metabolism — MCQs

On this page
Which of the following conditions is characterized by a lack of genetically mediated VLDL overproduction?
What is the parameter that is used to assess lipid peroxidation?
X-linked adrenoleukodystrophy is a type of:
Which of the following is a transfatty acid?
Which of the following statements about beta oxidation of fatty acids is correct?
All are true about beta oxidation of fatty acids except which of the following?
Which of the following statements about reverse cholesterol transport is false?
In congenital adrenal hyperplasia, which enzyme deficiency is primarily responsible for precocious puberty in males?
Lipoprotein involved in reverse cholesterol transport?
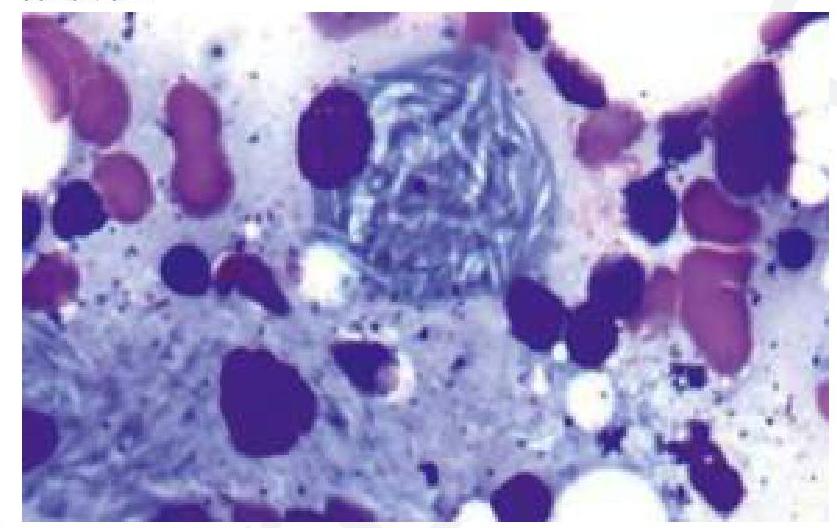
A child presents with bone pain and hepatosplenomegaly. A trephine biopsy and aspirate show the following finding. Which of the following is the most likely enzyme deficient in this condition?
Practice by Chapter
Lipid Classification and Chemistry
Practice Questions
Fatty Acid Oxidation
Practice Questions
Ketone Body Metabolism
Practice Questions
Fatty Acid Synthesis
Practice Questions
Metabolism of Triacylglycerols
Practice Questions
Phospholipid Metabolism
Practice Questions
Cholesterol Metabolism and Biosynthesis
Practice Questions
Bile Acids and Bile Salts
Practice Questions
Lipoprotein Metabolism and Transport
Practice Questions
Dyslipidemias and Atherosclerosis
Practice Questions
Prostaglandins and Eicosanoids
Practice Questions
Fatty Liver and Lipotropic Factors
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app