
Lipid Metabolism — MCQs

On this page
A child presents with hepatosplenomegaly & cherry red spots in the eye. He also has developmental regression with normal startle response. Likely enzyme deficiency?
A patient presents with elevated total cholesterol, subcutaneous xanthomas, and a positive family history of similar findings. Triglyceride levels are normal (<140 mg/dL). What is the most likely type of familial dyslipidemia?
A neonate presents with seizures and is found to have a cherry red spot on fundus examination. Enzyme assay reveals deficiency of hexosaminidase A. Which of the following substances is most likely to be accumulated in this patient?
A patient presents with orange-colored tonsils. Laboratory investigations reveal triglyceride level of 140 mg/dL and HDL cholesterol of 5 mg/dL. What is the most likely diagnosis?
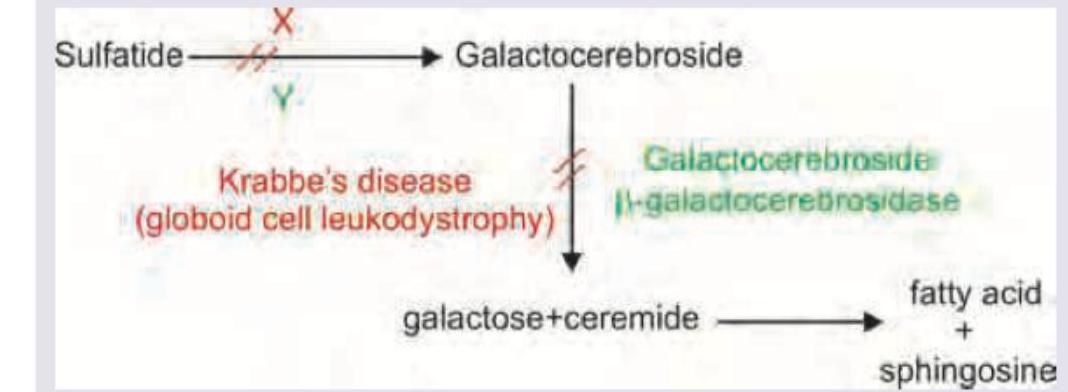
Which of the following is correct about the disease and its missing enzyme mentioned below?
A patient has a family history positive for premature coronary artery disease. All are true about the disease shown in the image, except?

Consider the following statements with reference to 'trans fatty acids' : 1. They are geometrical isomers of cis-unsaturated fatty acids. 2. Though atherogenic, being unsaturated they are less so than saturated fatty acids. 3. It takes years for trans fatty acids to be flushed from the body. 4. They lower both LDL cholesterol and HDL cholesterol in the body. Which of the statements given above are correct ?
Which of the following are unsaturated fatty acids? 1. Lauric acid 2. Linoleic acid 3. Oleic acid 4. Palmitic acid Select the correct answer using the code given below.
Which of the following fats has the highest concentration of saturated fatty acids ?
Which one of the following is a polyunsaturated fatty acid ?
Practice by Chapter
Lipid Classification and Chemistry
Practice Questions
Fatty Acid Oxidation
Practice Questions
Ketone Body Metabolism
Practice Questions
Fatty Acid Synthesis
Practice Questions
Metabolism of Triacylglycerols
Practice Questions
Phospholipid Metabolism
Practice Questions
Cholesterol Metabolism and Biosynthesis
Practice Questions
Bile Acids and Bile Salts
Practice Questions
Lipoprotein Metabolism and Transport
Practice Questions
Dyslipidemias and Atherosclerosis
Practice Questions
Prostaglandins and Eicosanoids
Practice Questions
Fatty Liver and Lipotropic Factors
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app