
Lipid Metabolism — MCQs

On this page
How many ATPs are formed from the complete beta-oxidation of stearic acid?
A 8-year-old child has a history since early childhood of malabsorption, ataxia, acanthocytes in the peripheral blood, and very low cholesterol and triglyceride levels. In addition, the patient has been developing progressive, bilateral, concentric contraction of the visual fields and loss of central vision. What is the underlying pathogenesis of this patient's disease?
Which oil contains the maximum proportion of unsaturated fatty acids?
Niemann-Pick disease is due to deficiency of which enzyme?
Acetyl-CoA is transported out of the mitochondria to serve as a substrate for fatty acid or cholesterol synthesis. Which of the following enzymes involved in this transport process provides NADPH required for these reductive biosynthesis reactions?
What is the best marker for the prediction of coronary artery disease?
Refsum's disease is due to the accumulation of which substance?
Which one of the following is a precursor of both gonadal and adrenocortical hormones?
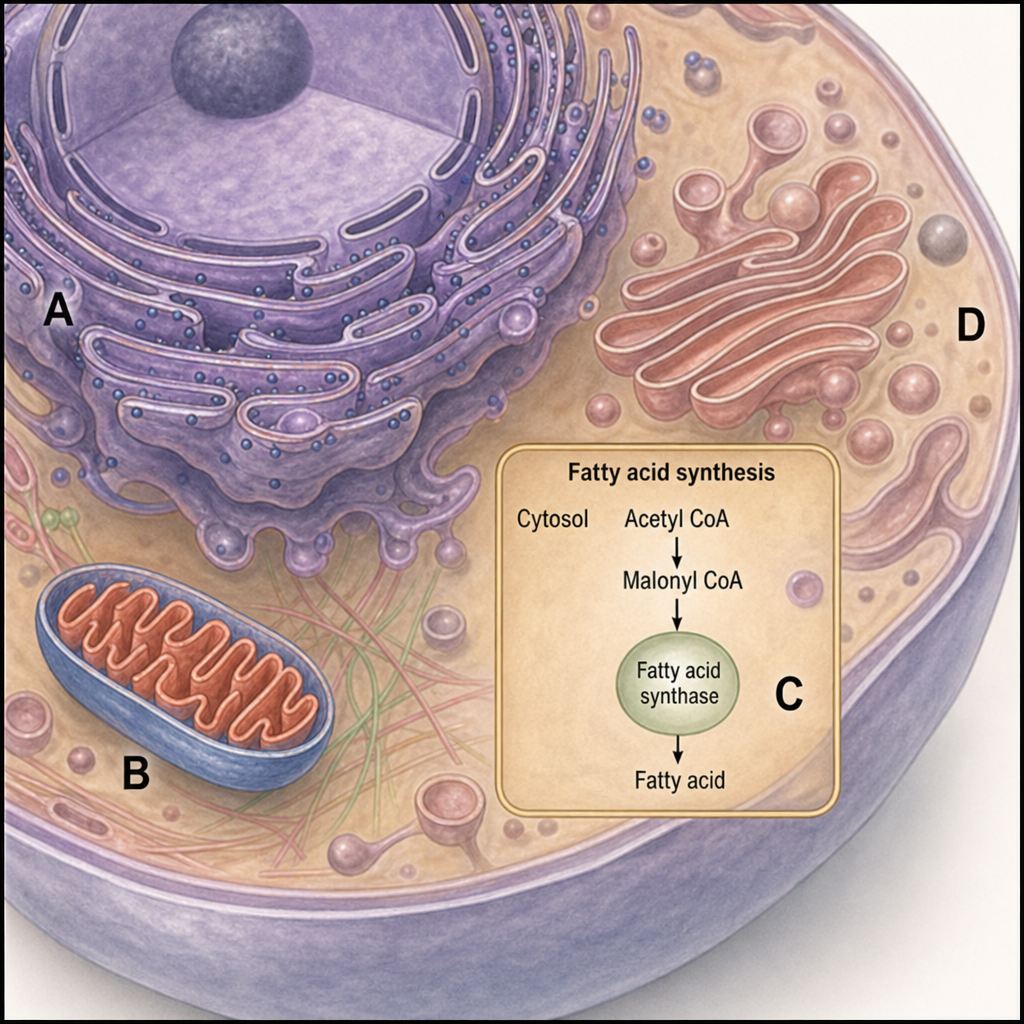
The elongation of fatty acids occurs in which of the diagrammatic structures shown in the illustration?
Which of the following is not an essential unsaturated fatty acid?
Practice by Chapter
Lipid Classification and Chemistry
Practice Questions
Fatty Acid Oxidation
Practice Questions
Ketone Body Metabolism
Practice Questions
Fatty Acid Synthesis
Practice Questions
Metabolism of Triacylglycerols
Practice Questions
Phospholipid Metabolism
Practice Questions
Cholesterol Metabolism and Biosynthesis
Practice Questions
Bile Acids and Bile Salts
Practice Questions
Lipoprotein Metabolism and Transport
Practice Questions
Dyslipidemias and Atherosclerosis
Practice Questions
Prostaglandins and Eicosanoids
Practice Questions
Fatty Liver and Lipotropic Factors
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app