
Enzyme Regulation: Zymogen Activation — MCQs

Digestion of proteins is initiated by:
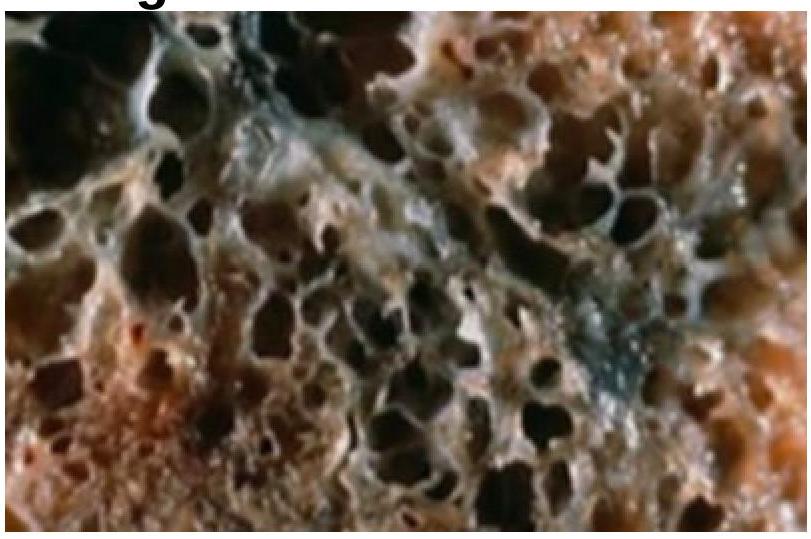
A patient presents with respiratory distress and is diagnosed with panacinar emphysema. Which of the following is deficient?
Which of the following statements best describes the mechanism of action of insulin on target cells?
A 35-year-old woman with a long history of dyspnea, chronic cough, sputum production, and wheezing dies of respiratory failure following a bout of lobar pneumonia. She was not a smoker or an alcoholic. Which of the following underlying conditions is most likely associated with the pathologic changes shown in the lung autopsy?
Inactive precursors of enzymes are known as:
All of the following are true about blood coagulation, except which of the following?
Which of the following is an example of allosteric inhibition?
How do enzymes function in biochemical reactions?
Enzyme activity is expressed as?
What is the specific activity of an enzyme?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app