
Chest Trauma Management — MCQs

A Patient presented to emergency with multiple rib fractures. He is conscious speaking single words. On examination, respiratory rate was 40/minute and BP was 90/40 mmHg. What is immediate next step?
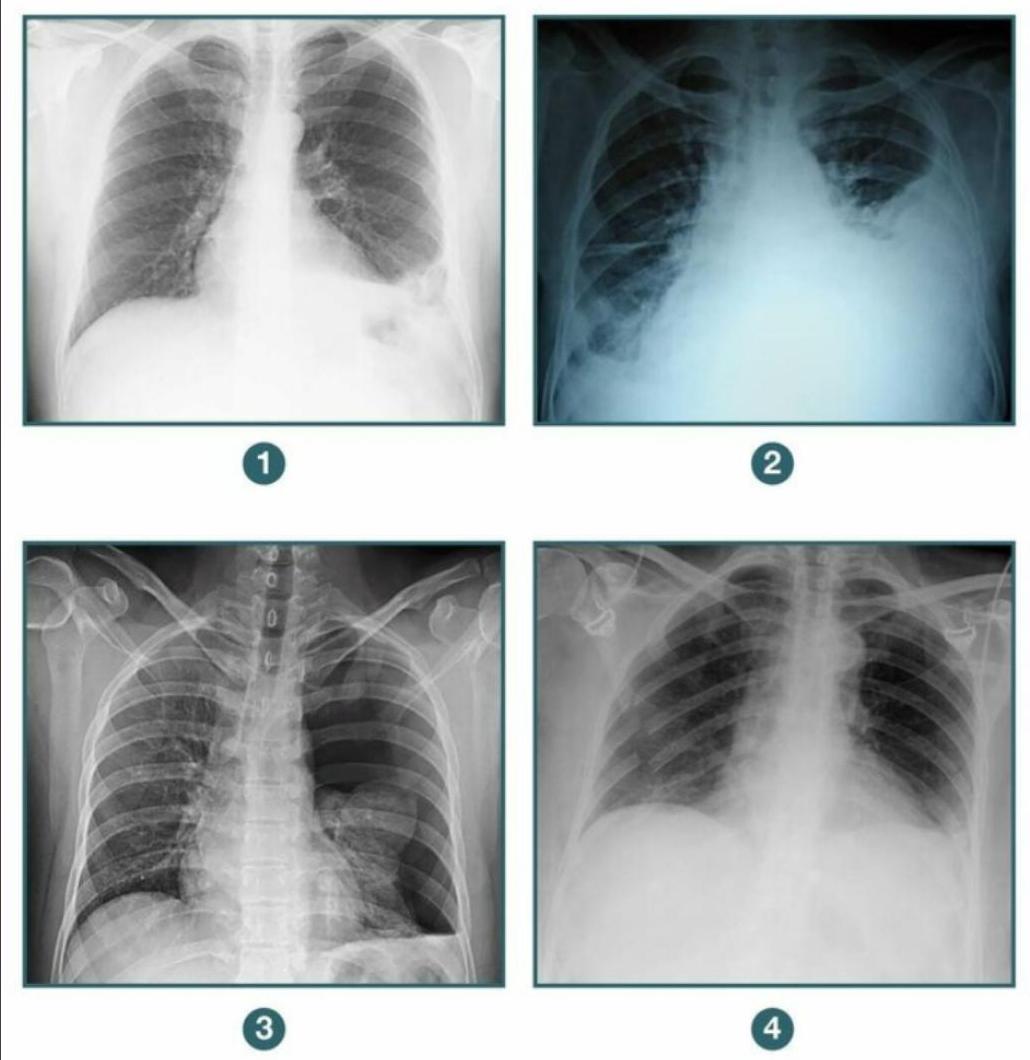
A patient presents to the casualty following blunt trauma to the chest. A chest X-ray was done. Among the following radiographs, in which case would you further evaluate the patient before putting a chest tube? 1. Diaphragmatic hernia 2. Hemothorax 3. Pneumothorax 4. Flail chest
Road traffic accident (RTA) with multiple fractures - initial treatment would be:
Indications for emergency thoracotomy are all of the following except:
A **hemodynamically stable** patient involved in a Road Traffic Accident (RTA) presents with: - Absent air entry on the left side of the chest. - Tenderness in the left lower chest wall. What is the next step in the Emergency Medicine Room (EMR) management?
What is to be addressed first in case of polytrauma -
A patient is admitted following a road traffic accident. He has sustained significant blunt injury to his head, chest and abdomen and has a Glasgow Coma Scale score of 8/15. His saturations are poor at 89% on 15 L of oxygen a rebreathing mask. You note bruising around both eyes and blood-stained fluid issuing from his left ear, which forms concentric circles when dripped on a white sheet. You wish to support his airway to improve oxygenation. The first choice of airway adjunct would be
Endotracheal tube in the esophagus is best assessed by:
Which of the following is an ideal method to prevent aspiration pneumonia?
Which of the following parameters is most critical for maintaining optimal oxygenation?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app