
One-Lung Ventilation Techniques — MCQs

Which of the following surgical incisions is associated with the highest risk of postoperative pulmonary complications ?
What happens to gas exchange when the Va/Q ratio approaches infinity?
At the end of anaesthesia after discontinuation of nitrous oxide and removal of endotracheal tube, 100% oxygen is administered to the patient to prevent:
Procedure of choice for control of massive hemoptysis?
Which of the following is not true about ventilation-perfusion ratio (V/Q)?
Identify the instrument shown in the image:
A man is brought to casualty who met with an accident. He sustained multiple rib fractures with paradoxical movement of chest. Management is:
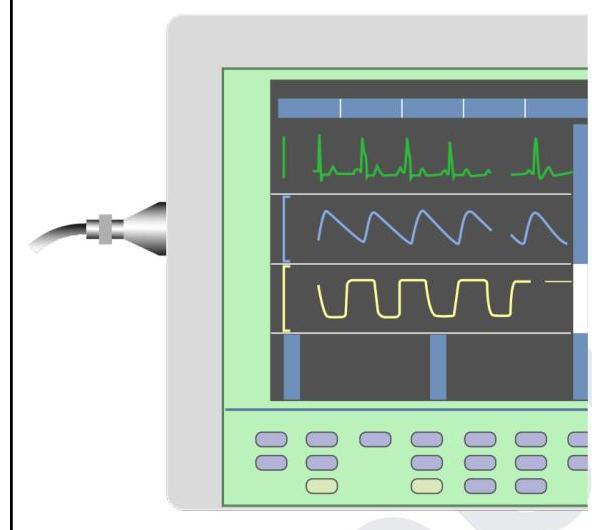
You are in the operating room and notice the tracing in yellow colour on this device. What does it indicate?
A 10-year-old boy, unconscious with 2 days history of fever, comes to pediatric ICU with respiratory rate 46/min, blood pressure 110/80 mmHg, and Glasgow Coma Scale E1 V1 M3. The next step in management is
A 30-year-old male was intubated for surgery. What is the best method to confirm the correct position of the endotracheal tube?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app