
Preoperative Evaluation and Management — MCQs

On this page
Which of the following drugs is contraindicated in a patient with myasthenia gravis?
What is true about Ringer's Lactate?
Which patient has the least risk of pulmonary aspiration of gastric contents during induction of anesthesia?
A patient scheduled for elective hip surgery is currently taking aspirin, enalapril, a multivitamin, and metoprolol. The surgery is planned in 5 days. What is the appropriate perioperative management for this patient?
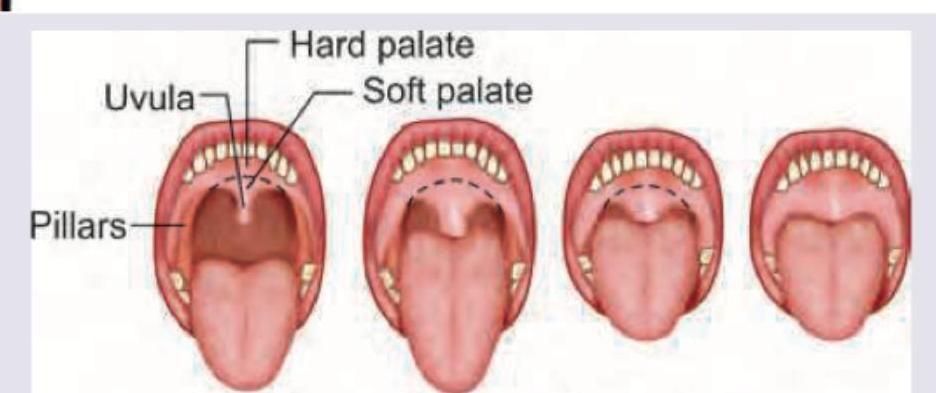
Which of the following is the use of the Mallampatti classification?
What is this classification used for?
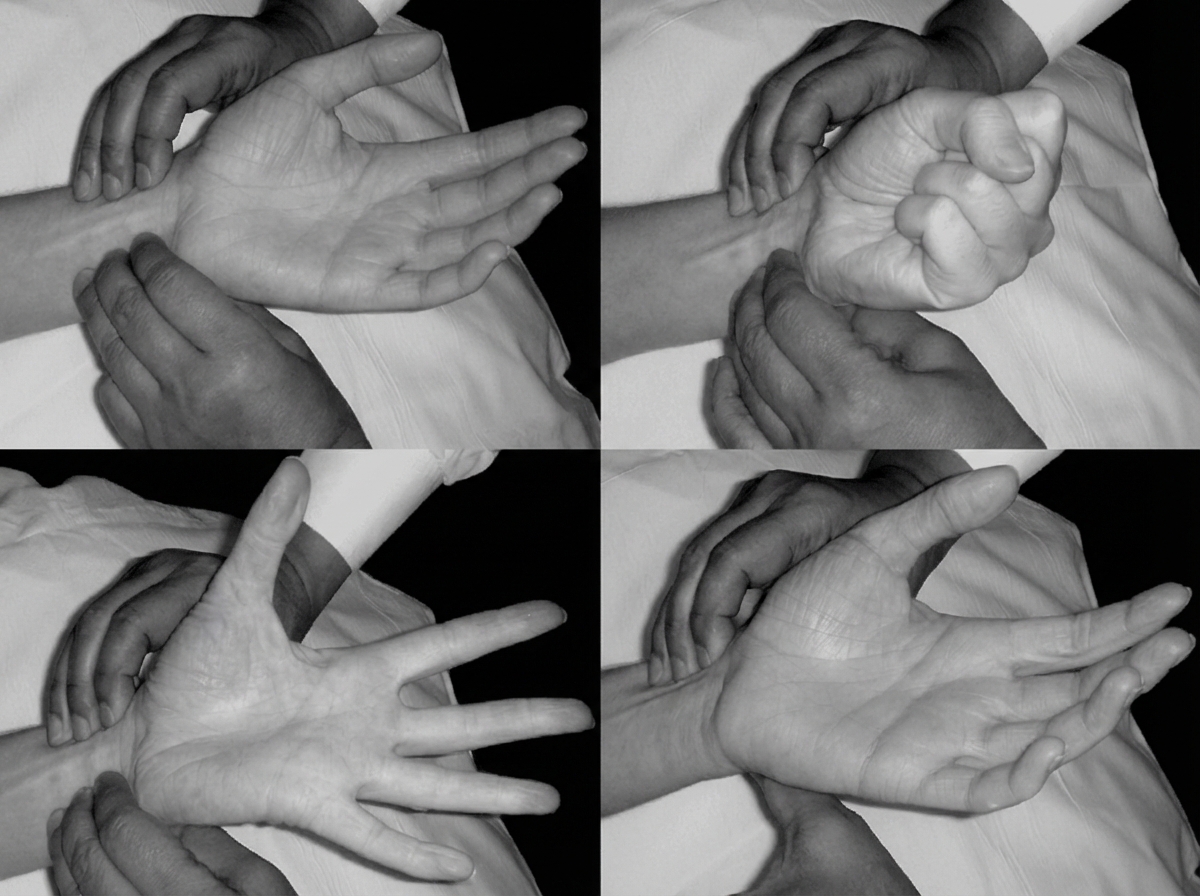
Identify the test performed in the image:
A 56-year-old female has been diagnosed with gallstones and is undergoing a preanaesthesia checkup. She has been a diabetic since last 15 years, but sugar levels are within the limits. Which category of physical status does she fit into?
Perioperative benefit from transfusion is with a haemoglobin level of
Preoperative Samsoon and Young modified, Mallampati test is used for assessing:
Practice by Chapter
Preoperative Assessment Framework
Practice Questions
ASA Physical Status Classification
Practice Questions
Preoperative Laboratory Testing
Practice Questions
Cardiovascular Evaluation
Practice Questions
Pulmonary Evaluation
Practice Questions
Assessment of the Difficult Airway
Practice Questions
Medication Management
Practice Questions
NPO Guidelines
Practice Questions
Perioperative Anticoagulation Management
Practice Questions
Premedication
Practice Questions
Informed Consent
Practice Questions
Risk Stratification
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app