
Opioid-Sparing Analgesia — MCQs

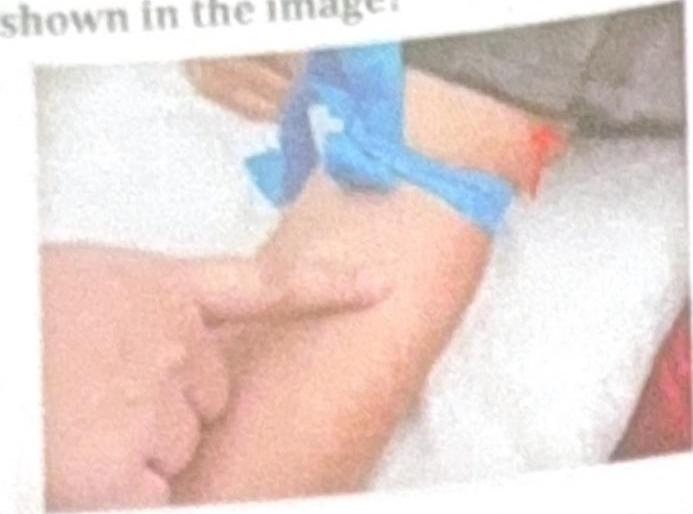
What is the name of the nerve block technique shown in the image?
Match the following: A) Glossopharyngeal nerve B) Spinal accessory nerve C) Facial nerve D) Mandibular nerve 1) Shrugging of shoulder 2) Touch sensation from the posterior one-third of the tongue 3) Chewing 4) Taste from the anterior two-thirds of the tongue
Which of the following anaesthetic agent lacks analgesic effect? A) N2O B) Thiopentone C) Methohexitone D) Ketamine E) Fentanyl
Which of the following anesthetic agents have good analgesic property? a) Ketamine b) Nitrous oxide c) Thiopentone d) Propofol e) Midazolam
Which of the following is an example of placebo?
Which drug is commonly used for outpatient department (OPD) analgesia?
A 35-year-old woman presents with a history of recurrent migraines, unresponsive to prophylactic medications. What is the most appropriate next step in management?
Which Benzodiazepine decreases post-operative nausea & vomiting:-
Which opioid drug is effectively administered via the transbuccal route?
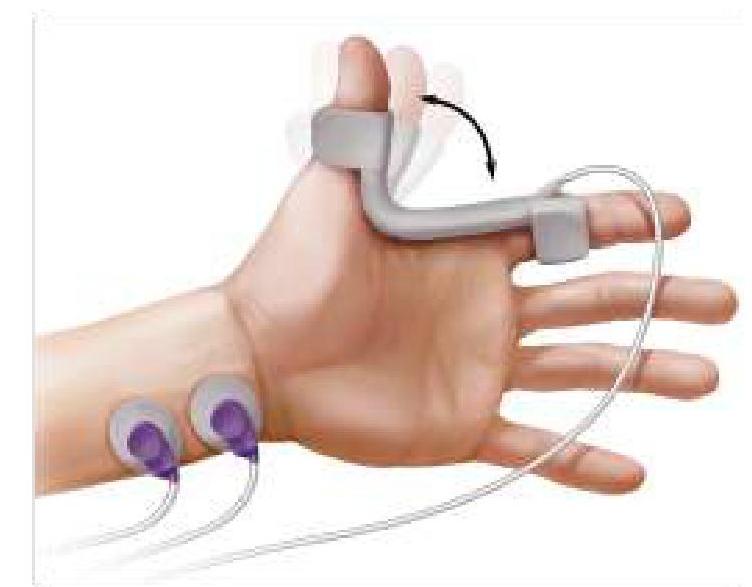
The image given below shows neuromuscular monitoring of the patient after anesthesia. What is the most commonly used nerve for monitoring?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app