
Mechanical Ventilation Principles — MCQs

Which of the following is measured by the Bellows spirometer?
Which lung volume cannot be measured by spirometry?
Which of the following parameters indicates the elimination of CO2 from the lungs?
Patient of pneumonia on ventilator with wt. 50 kg. RR 14/min, bicarbonate - 18, pH 7.3, pCO2 48 mmHg, pO2 110 mmHg, PEEP 12 cm H2O, tidal volume 420 mL, SpO2 - 100% with FiO2 90%. What is next step in management?
Risk of adverse effects of SCOLINE is greater in
Which of the following is markedly decreased in restrictive lung disease?
Which of the following is not a risk factor for postoperative pulmonary complication?
In which of the following conditions is Positive end-expiratory pressure (PEEP) beneficial?
Which of the following is not a known complication associated with the procedure done in the patient?

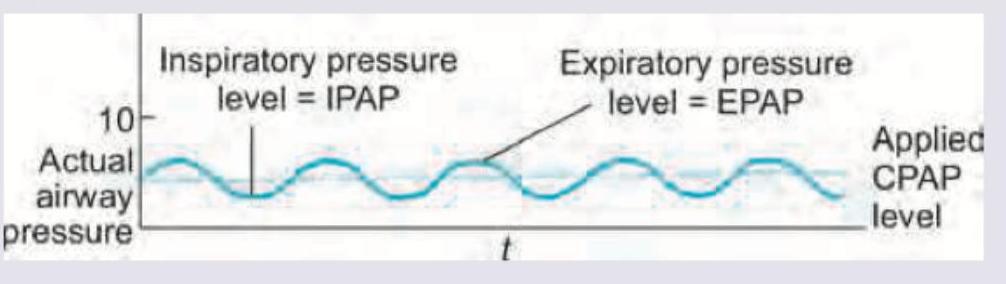
The following ventilation modality is used in:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app