
Safety Considerations in Non-Operating Room Anesthesia — MCQs

In an accident case, after the arrival of medical team, all should be done in early management except;
Child with aspiration risk needs emergency surgery. Best induction sequence is:
True about anesthesia cylinders is all EXCEPT:
Which of the following is not done in the primary survey of trauma?
A 50 year old male is posted for elective laparoscopic cholecystectomy. No history of comorbidities. His surgery is scheduled at 2 PM on the day of surgery. Which of the following is against the ASA guidelines for preoperative fasting
Depth of Anesthesia is best measured by:
All are absolute contraindication of neuraxial anaesthesia except:
A moribund patient unlikely to survive 24 hours without surgery is classified as
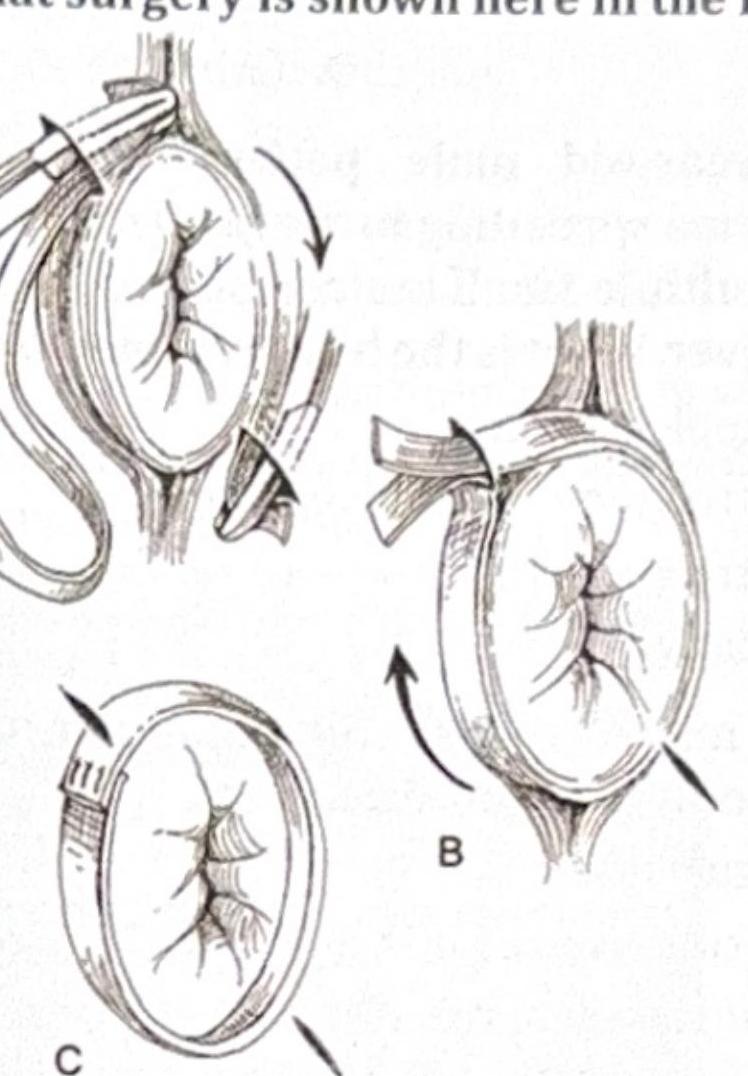
What surgery is shown here in the image?
Surgery of choice in a patient with congenital ptosis with good levator action is:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app