
Anesthesia for Thoracic Emergencies — MCQs

Thoracotomy is indicated in all the following conditions except:
A patient after undergoing thoracotomy complains of severe pain. The BEST method of pain control in this patient would be:
What type of respiratory failure is most commonly observed in post-operative patients?
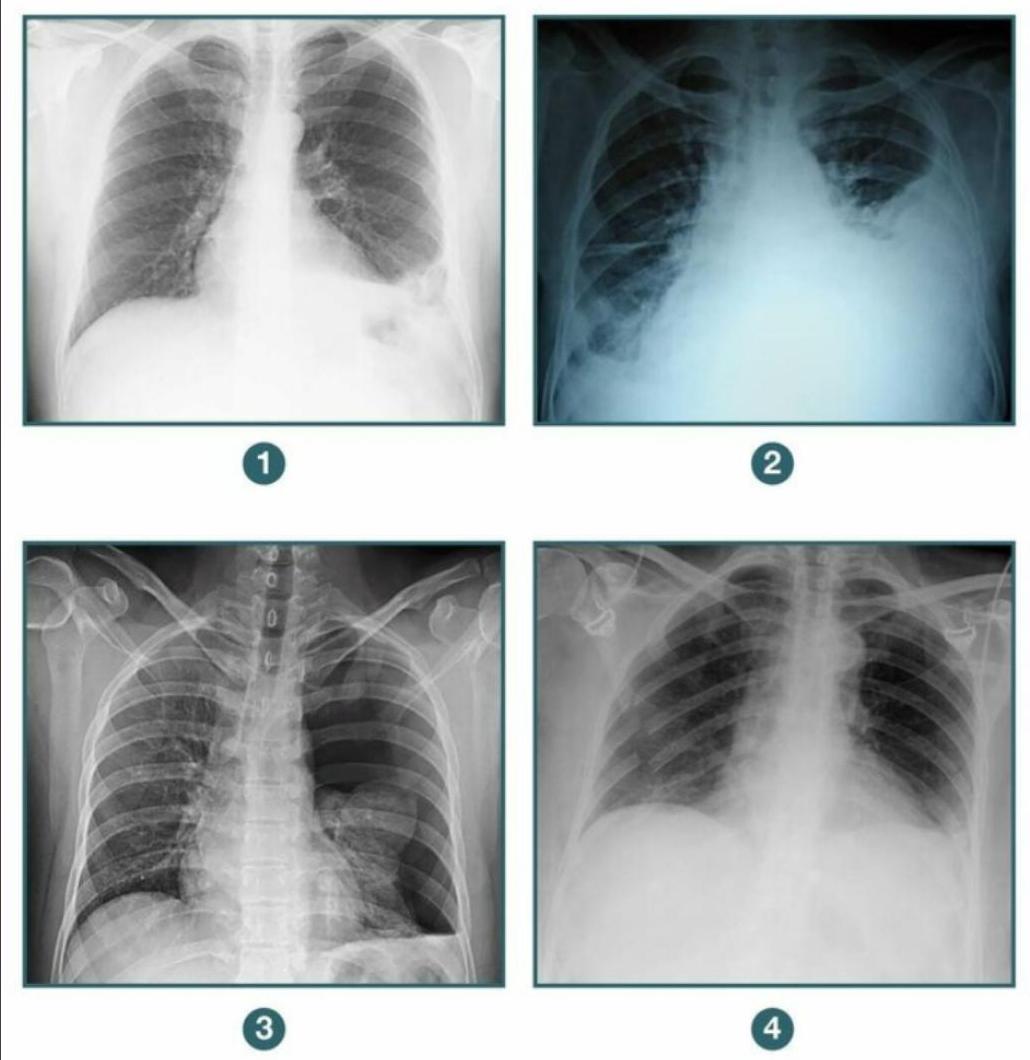
A patient presents to the casualty following blunt trauma to the chest. A chest X-ray was done. Among the following radiographs, in which case would you further evaluate the patient before putting a chest tube? 1. Diaphragmatic hernia 2. Hemothorax 3. Pneumothorax 4. Flail chest
Road traffic accident (RTA) with multiple fractures - initial treatment would be:
Indications for emergency thoracotomy are all of the following except:
All are indications for one-lung ventilation except which of the following?
Child with aspiration risk needs emergency surgery. Best induction sequence is:
What is an absolute indication for surgery in disc prolapse?
Identify the airway device shown in the image.

Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app