
Thoracic Imaging and Cross-sectional Anatomy — MCQs

Best imaging modality for acute pulmonary embolism
Which of the following segments is present in the middle lobe of the right lung?
A 60-year-old male presents with sudden onset of pleuritic chest pain and dyspnea. Chest X-ray shows a wedge-shaped opacity in the lung. What is the most likely diagnosis?
Which of the following statements regarding axillary lymph nodes is incorrect?
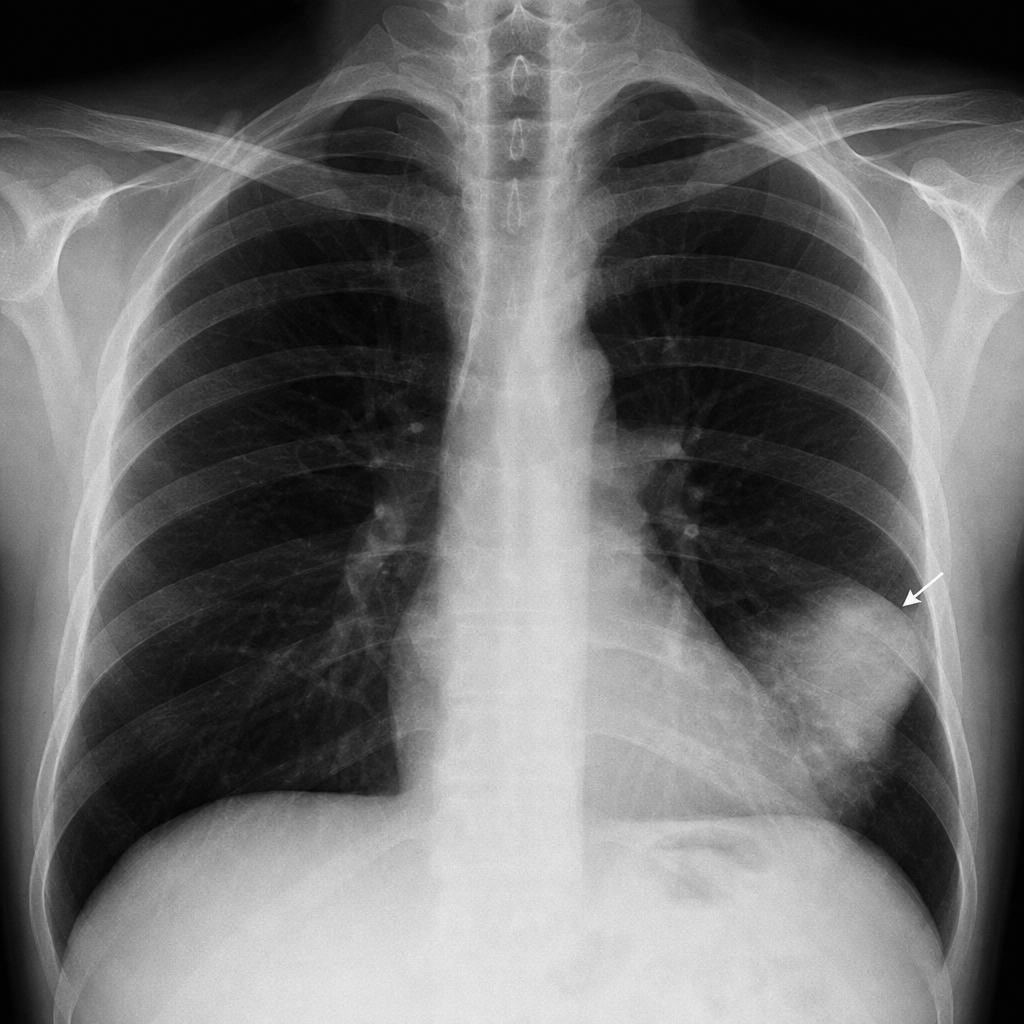
A chest X-ray shows a 'silhouette sign' with opacity obscuring the right heart border. Which lobe of the lung is most likely affected?
The thoracic duct crosses from the right to the left at the level of
The incidence of a foreign body being aspirated into the right lung is higher than into the left lung. All of the following statements support this, EXCEPT?
Carina is situated at which level?
Which of the following statements about the atrioventricular groove is true?
The aortic hiatus is formed by the right and left crura of the diaphragm. Which of the following structures does NOT pass through the aortic hiatus?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app