
Sectional and Cross-sectional Anatomy — MCQs

The aortic hiatus is formed by the right and left crura of the diaphragm. Which of the following structures does NOT pass through the aortic hiatus?
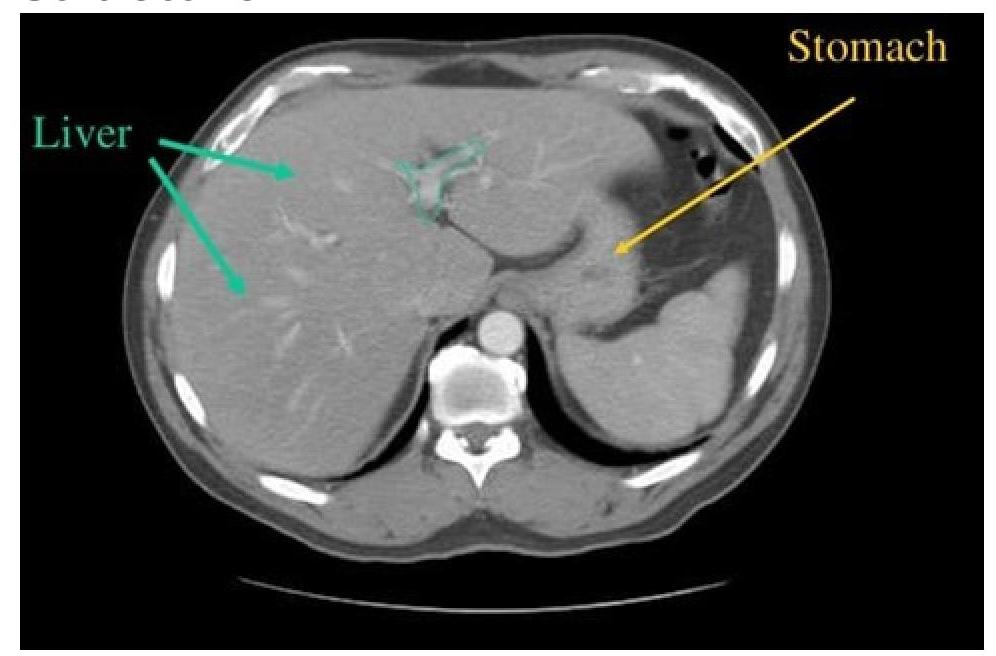
CT scan of abdomen showing a structure branching within the liver. Identify the structure.
When a lumbar puncture is performed to sample cerebrospinal fluid, which of the following external landmarks is the most reliable to determine the position of the L4 vertebral spine?
Which artery is the major supply of the medial surface of the cerebral hemisphere?
To visualize vascular sling causing tracheal or external airway compression, which of the following would you best prefer?
Which structure is not seen at the L3 level?
Blumensaat line is used to radiologically diagnose an anatomical condition called patella alta. It is
Which CT view is best for visualizing paranasal polyps?
Which type of study determines the odds ratio?
Which research method is most appropriate for studying the progression of a disease over time?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app