
Head — MCQs

On this page
Post-tonsillectomy, a patient experiences altered taste and impaired swallowing. Evaluate the nerve that is likely affected and the subsequent impact on its functions.
A surgical team is concerned about nerve injury during parotid gland tumor resection. Which nerve is most at risk of injury during this surgery?
During a dissection, a medical student has difficulty tracing the facial nerve through the parotid gland. What anatomical relationships should they consider to accurately locate this nerve?
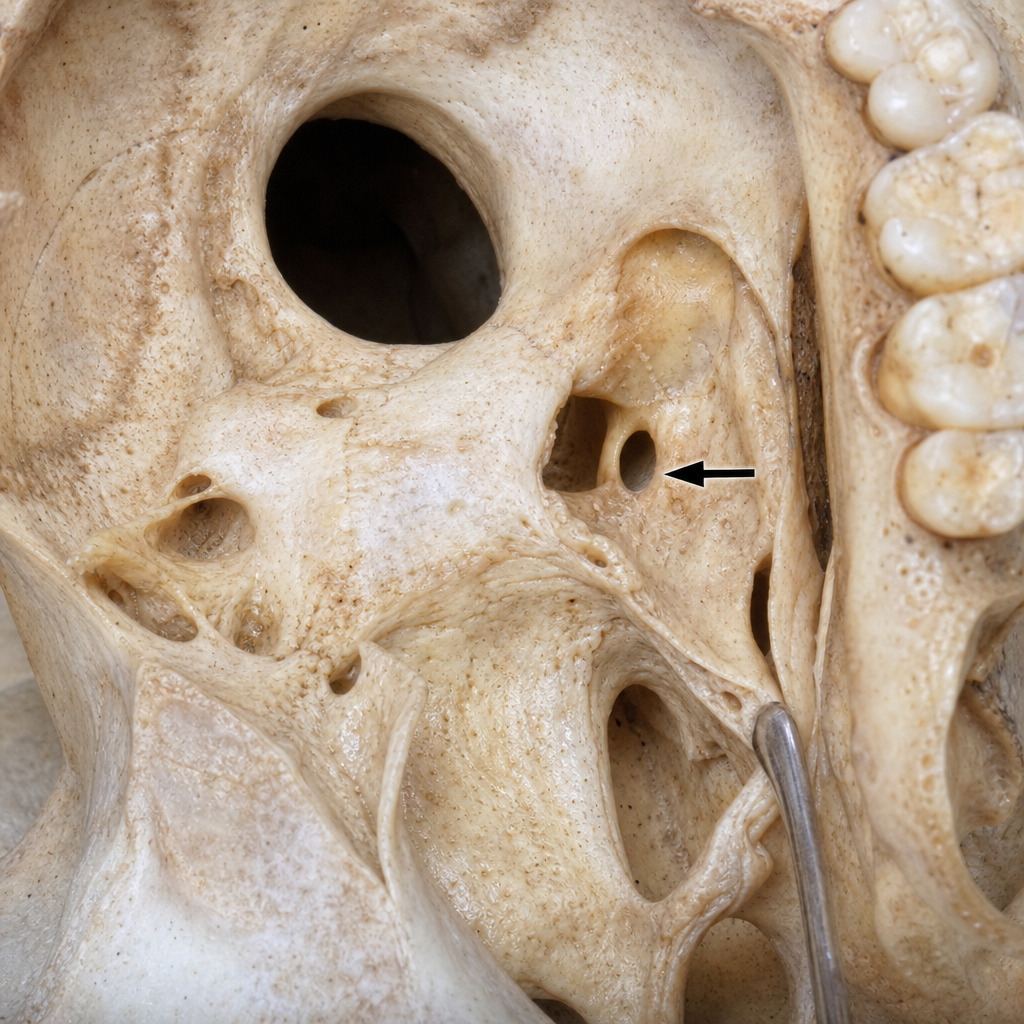
Which nerve passes through the marked foramen in the image?
MacEwen's triangle is the landmark for:
What is the anatomical significance of the Agger nasi?
Quadrangular cartilage is seen in which of the following anatomical structures?
In which part of the inner ear are cristae located?
Which of the following is the primary mechanical action of the tensor tympani muscle?
Partial ptosis due to oculomotor nerve injury is due to intact what?
Practice by Chapter
Skull and Facial Bones
Practice Questions
Scalp and Facial Muscles
Practice Questions
Dural Venous Sinuses
Practice Questions
Cranial Cavity
Practice Questions
Orbit and Contents
Practice Questions
Temporal and Infratemporal Regions
Practice Questions
Pterygopalatine Fossa
Practice Questions
Oral Cavity
Practice Questions
Paranasal Sinuses
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app